

Abstract
Systemic mastocytosis (SM) is a hematologic neoplasm characterized by abnormal expansion and accumulation of neoplastic mast cells (MC) in various organs, including the bone marrow, skin, liver, spleen and gastrointestinal tract. In a majority of all patients, the transforming KIT mutation D816V is detectable. The clinical picture and prognosis in SM vary, depending on the variant of SM and the presence of an associated hematologic non-MC-lineage disease (AHNMD). The WHO classification discriminates between indolent SM (ISM), SM-AHNMD, aggressive SM (ASM) and MC leukemia (MCL). Recent data suggest that neoplastic MC in ASM and MCL express substantial amounts of cytoplasmic Ki-1 (CD30), a lymphoid antigen otherwise expressed in neoplastic cells in anaplastic large cell lymphoma and Hodgkin lymphoma, where CD30 serves as a therapy target. In the present study, we examined the expression of CD30 in various human MC-lines (HMC-1, MCPV) and primary neoplastic MC in patients with ISM (n=20) and advanced SM (ASM/MCL; n=10) and asked whether CD30 may serve as potential therapeutic target in SM. We found that CD30 is expressed abundantly in the cytoplasm of neoplastic MC in ASM and MCL in almost all patients, whereas in a majority of patients with ISM, MC expressed only low amounts or did not express cytoplasmic CD30. As assessed by flow cytometry, neoplastic MC in SM were also found to express cell surface CD30. In contrast to cytoplasmic expression, no clear correlation was found between the type of SM and CD30 surface expression on MC. Notably, MC expressed surface CD30 in 8/9 ISM patients and in 2/6 ASM/MCL patients. The immature human RAS-transformed MCL line MCPV (KIT D816V negative) also expressed cell surface CD30, whereas the MCL line HMC-1.1 (lacking KIT D816V) expressed only low levels, and the HMC-1.2 subclone (KIT D816V+) was found to stain CD30 negative. To examine whether CD30 may serve as a therapy target in SM, we applied brentuximab vedotin (provided by Millennium: The Takeda Oncology Company, Cambridge, MA, USA), which is an antibody-drug conjugate consisting of a chimeric anti-CD30 antibody and the microtuble inhibitor monomethyl auristatin E (MMAE). Brentuximab vedotin has recently been described to induce dose-dependent growth arrest in human CD30+ lymphoblastic cell lines. In the present study, brentuximab vedotin was found to inhibit the proliferation of MCPV and HMC-1 cells in a dose-dependent manner, with lower IC50 values found in CD30+ MCPV and HMC-1.1 cells (5 µg/ml) than in CD30− HMC-1.2 cells (10 µg/ml). As assessed by AnnexinV/PI staining and staining for active-caspase-3, brentuximab vedotin also induced dose-dependent apoptosis in CD30+ MCPV and HMC-1.1 cells, but did not induce substantial apoptosis in CD30− HMC-1.2 cells. Brentuximab vedotin was also found to induce growth inhibition and apoptosis in the CD30+ canine-mastocytoma cell line C2. We next examined the effects of brentuximab vedotin on in vitro survival (apoptosis) of primary neoplastic MC in patients with CD30− SM (n=3) and in patients with CD30+ SM (n=3). In these experiments, brentuximab vedotin was found to induce dose-dependent apoptosis at pharmacologically relevant concentrations in neoplastic MC in patients with CD30+ SM, whereas no effects were seen in patients with CD30− SM (Figure). Finally, we examined the effects of a drug combination consisting of brentuximab vedotin and the KIT D816V targeting drug PKC412 (midostaurin). We found that both drugs synergize with each other in inhibiting the in vitro proliferation of CD30+ MCPV cells. In conclusion, our data provide evidence that the target-antigen CD30 is expressed on the surface of neoplastic MC in patients with indolent and advanced SM. In addition, our data show that the CD30-targeting antibody brentuximab vedotin induces growth arrest and apoptosis in neoplastic MC and synergizes with midostaurin in inhibiting the growth of CD30+ neoplastic MC. Whether these effects also occur in vivo in patients with advanced mastocytosis remains to be determined in clinical trials.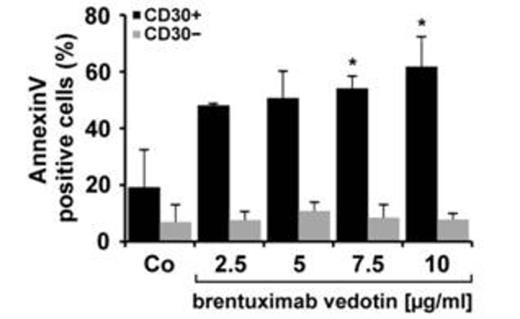

Neoplastic MC from patients with CD30− SM (n=3, grey bars) and CD30+ SM (n=3, black bars) were incubated in control medium (Co) or in various concentrations of brentuximab vedotin (37°C). After 96 hours, the percentage of AnnexinV+ viable DAPI-negative MC was determined by flow cytometry. Results represent the mean±S.D. of 3 independent experiments. Asterisk: p<0.05 compared to control.
Disclosures:
Sotlar:Nanostring: Honoraria; Novartis: Consultancy. Reiter:Novartis: Consultancy, Honoraria. Horny:Novartis: Consultancy, Honoraria. Valent:Novartis: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal