Key Points
Public demographic reporting for acute leukemia trials is inadequate, and NH-White subjects are more likely to be enrolled.
Larger racial-ethnic enrollment disparities were documented after federal reporting requirements, which may be from more data transparency.

Abstract
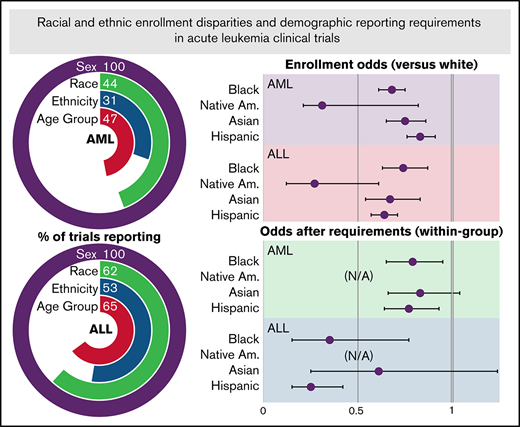
Data regarding racial and ethnic enrollment diversity for acute myeloid leukemia (AML) and acute lymphoid leukemia (ALL) clinical trials in the United States are limited, and little is known about the effect of federal reporting requirements instituted in the late 2000s. We examined demographic data reporting and enrollment diversity for ALL and AML trials in the United States from 2002 to 2017, as well as changes in reporting and diversity after reporting requirements were instituted. Of 223 AML trials and 97 ALL trials with results on ClinicalTrials.gov, 68 (30.5%) and 51 (52.6%) reported enrollment by both race and ethnicity. Among trials that reported race and ethnicity (AML, n = 6554; ALL, n = 4149), non-Hispanic (NH)-Black, NH-Native American, NH-Asian, and Hispanic patients had significantly lower enrollment compared with NH-White patients after adjusting for race-ethnic disease incidence (AML odds ratio, 0.68, 0.31, 0.75, and 0.83, respectively; ALL odds ratio, 0.74, 0.27, 0.67, and 0.64; all, P ≤ .01). The proportion of trials reporting race increased significantly after implementation of the reporting requirements (44.2% to 60.2%; P = .02), but race-ethnicity reporting did not (34.8% to 38.6%; P = .57). Reporting proportions according to number of patients enrolled increased significantly after the reporting requirements were instituted (race, 51.7% to 72.7%; race-ethnicity, 39.5% to 45.4%; both, P < .001), and relative enrollment of NH-Black and Hispanic patients decreased (AML odds ratio, 0.79 and 0.77; ALL odds ratio, 0.35 and 0.25; both P ≤ .01). These data suggest that demographic enrollment reporting for acute leukemia trials is suboptimal, changes in diversity after the reporting requirements may be due to additional enrollment disparities that were previously unreported, and enrollment diversification strategies specific to acute leukemia care delivery are needed.
Introduction
In the early 2000s, prominent analyses of cancer clinical trials reported significant disparities in enrollment according to race and ethnicity.1,2 Among National Cancer Institute Clinical Trial Cooperative Group medical oncology trials for breast, colorectal, lung, and prostate cancer from 2000 to 2002, adjusted enrollment for Black and Hispanic persons was 28% and 29% lower than for White subjects.1 In the Clinical Trial Cooperative Group surgical oncology trials for the same cancers and from the same period, enrollment disparities were even more substantial.2 Together, these studies suggested that enrollment inequities according to race and ethnicity were pervasive across multiple treatment modalities for common solid tumors.
Although restricting trial enrollment to ensure equipoise and scientific integrity is understandable,3,4 underrepresentation of demographic groups without justification is not. Indeed, such restrictions compound underlying inequities in several ways. First, clinical trials include additional clinician interactions and disease assessments that may actually result in higher quality care.5-7 Second, when underrepresented groups are not included in trials, the applicability of trial results to these patients is limited.8,9 Third, access to clinical trials is a moral imperative, as the treatments being tested are by definition at the forefront of clinical innovation and should be equally accessible to all. Finally, trial underrepresentation in a world of big data engenders further data absenteeism (ie, lack of data representation from underprivileged groups) and data chauvinism (ie, faith in the size of data without considerations for quality and contexts).8
In response, federal and medical society policies were introduced in the late 2000s aiming to reduce such disparities by promoting data transparency through public demographic reporting. These included FDAAA801,10 a federal act that required reporting of demographic enrollment data to ClinicalTrials.gov within 12 months of study completion, with monetary penalties of up to $10 000 per day and/or withholding of grant funds for noncompliance; the public release of these data on ClinicalTrials.gov11 ; and updates to the Declaration of Helsinki that considered public registration of trials and disclosure of enrollee demographic characteristics obligatory research practices.12 Little is known about disparities in enrollment and the effects of these policies on enrollment diversity for patients with acute myeloid leukemia (AML)13 or acute lymphoblastic leukemia (ALL), rare but potentially curable blood cancers with numerous idiosyncratic care patterns that likely influence enrollment; these care patterns include the short time from diagnosis to therapy initiation, the inpatient setting of treatment, the high proportion of tertiary or quaternary care, and the historic paucity of effective treatments.7,14
Acute leukemia disparities research has uncovered biologic factors, health behaviors, individual factors, and structural barriers that are associated with worse outcomes for Hispanic, non-Hispanic (NH)-Black, and NH-Asian persons compared with NH-White subjects.4,15-17 Some mediators of these differences are now beginning to be uncovered. They include racial and ethnic correlations with cytogenetics and mutational patterns,15,18 lower rates of treatment,19 higher levels of community poverty and lower levels of affluence,20 and public insurance.21 However, disparities in key processes of acute leukemia care delivery, such as clinical trial participation, remain unclear. Identifying these biases, and elucidating if prior efforts regarding enrollment performance feedback through data reporting were successful, are key to understanding how current data are limited, which populations should be approached to restore enrollment diversity, and how reporting and feedback interventions might be useful.22
Unless enrollment disparities are systematically characterized and addressed, biased drug development and care delivery will continue to impede cancer control for historically disadvantaged groups.23,24 To better understand the distribution of acute leukemia trial enrollment and the potential ameliorative effect of data reporting requirements, we analyzed racial and ethnic enrollment patterns for US clinical trials through a structured abstraction of ClinicalTrials.gov, comparing these results to the demographic distributions of AML and ALL in the United States.
Methods
Clinical trial enrollment
We queried ClinicalTrials.gov25 with 2 separate searches, using the terms “acute myeloid leukemia” and “acute lymphoid leukemia,” respectively, with start and primary completion dates between January 1, 2002, and December 31, 2017. Interventional trials testing anticancer therapies were included. We reviewed publications associated with each clinical trial number on the MEDLINE database. For studies with incomplete demographic data and/or recruiting patients with other diseases or from other countries, we engaged primary study contacts for missing data; studies were excluded if the number of patients with AML and/or ALL enrolled at US sites could not be determined.
Disease incidence
Surveillance, Epidemiology, and End Results (SEER) data (SEER*Stat version 8.3.8)26 and the 2010 US Census data27 were used to determine the number of persons diagnosed with AML and ALL in each demographic category. We identified annual incidence for the years 2002 to 2017 via the SEER-21 data set by ICD-0-3/WHO-2008 site and pathology recode categories of “acute myeloid leukemia” and “acute monocytic leukemia” for AML and “acute lymphoblastic leukemia” for ALL; counts were categorized according to age, year of diagnosis, and race/ethnicity, and duplicates were excluded. Census populations by age, race, and ethnicity for the total US population and each SEER registry were identified and subgroup proportions within registry areas calculated. Race and ethnicity data were reconciled into 5 mutually exclusive racial-ethnic categories of NH-White, NH-Black, NH-Asian, NH-Native American/Alaska Native (NA/AN), and Hispanic; persons reporting as more than one race were excluded.
Statistical analysis
We calculated enrollment fractions for each racial-ethnic category, defined as the number of trial enrollees within a subgroup over a given period divided by the estimated number of incident cases in that subgroup during the period.1 Enrollment fractions according to racial-ethnic category were compared by using Pearson χ2 testing, with NH-White as the comparator group and reporting odds ratios with 95% confidence intervals. Additional analyses were performed by the study sponsor, as National Institutes of Health (NIH)-sponsored trials have been mandated to include racial and ethnic minorities in clinical research since 1993,11 and for pediatric and adult trials.
To assess the potential effect of the data transparency interventions, we compared the proportions of trials and of enrolled populations for which demographic characteristics were reported for periods before (2005-2008) and after (2011-2014) the policies were implemented by using two-sample, two-tailed z-tests; P < .05 was considered significant. To evaluate changes in enrollment diversity between these periods, enrollment within each racial-ethnic group was adjusted for changes in incidence and NH-White enrollment between the periods, and within-group enrollment odds ratios were calculated. The study was approved by the Dana-Farber Office for Human Research Studies and was conducted in accordance with the Declaration of Helsinki.
Results
The searches returned 260 completed studies with results reported in AML and 191 in ALL, with enrollment of 23 024 and 17 470 patients, respectively. The final number of trials included in the analysis was 223 for AML and 97 for ALL; search results and exclusions are shown in Figure 1. The final trial populations of 17 372 (AML) and 7968 (ALL) patients constituted 9.3% and 11.7% of incident cases over the study period, assuming mutual exclusivity of enrollment. Demographic reporting percentages for AML and ALL trials are also shown in Figure 1; 68 AML trials (30.5%) and 51 ALL trials (52.6%) reported both race and ethnicity. The proportions of clinical trials that reported age, race, and ethnicity demographic characteristics were higher for ALL than AML.

ClinicalTrials.gov search results schema and demographic reporting proportions for included trials. Excluded trials are shown in the green boxes and were excluded for not reporting results (top) or for the specific reason listed (bottom). Demographic reporting proportion comparisons (blue box) were performed between AML and ALL trial and patient proportions by using two-sided z-tests.
ClinicalTrials.gov search results schema and demographic reporting proportions for included trials. Excluded trials are shown in the green boxes and were excluded for not reporting results (top) or for the specific reason listed (bottom). Demographic reporting proportion comparisons (blue box) were performed between AML and ALL trial and patient proportions by using two-sided z-tests.
Table 1 describes the incidence, enrollment proportions, and enrollment fractions according to race-ethnicity for studies reporting race and ethnicity data within each acute leukemia subtype. In both AML and ALL, NH-White patients were more likely to be enrolled compared with NH-Black, NH-Asian, NH-NA/AN, and Hispanic patients. Figure 2 shows a forest plot of enrollment fraction odds ratios for NH-Black, NH-Asian, NH-NA/AN, and Hispanic subjects compared with NH-White subjects according to trial sponsor and patient age group. NIH sponsorship of trials led to odds of enrollment that were not significantly lower for NH-NA/AN and Hispanic subjects with AML and NH-Black and NH-Asian subjects with ALL (all, P > .05). With the exception of NH-Black patients with ALL enrolled into pediatric trials, all other age-based subgroups had significantly lower odds of enrollment compared with NH-White subjects (all, P < .05).
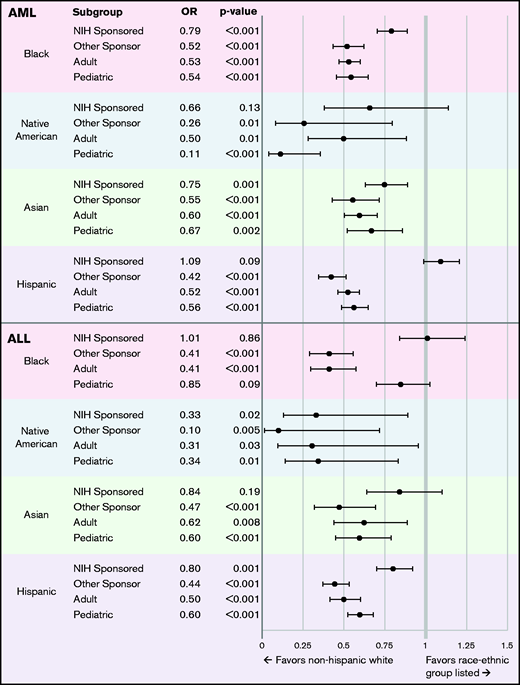
Forest plot of enrollment fraction odds ratios (ORs) compared with NH-White subjects according to trial sponsor and patient age group enrolled. Shown are 95% confidence intervals.
Forest plot of enrollment fraction odds ratios (ORs) compared with NH-White subjects according to trial sponsor and patient age group enrolled. Shown are 95% confidence intervals.
Changes in the proportions of the trials and enrolled populations for which race and race-ethnicity were reported before (2005-2008) and after (2011-2014) the reporting requirements were instituted are shown in Figure 3. According to trial (Figure 3A), reporting of race increased significantly (44.2% to 60.2% of trials; z-test, P = .02) but race-ethnicity reporting did not (34.8% to 38.6%; P = .57). Significant increases in racial demographic reporting were seen for AML trials (39.0% to 57.6%; P = .02) but not for ALL trials (60.0% to 70.8%; P = .36). Race-ethnicity reporting changes for trials were mixed between leukemia subtypes. Subgroup analyses according to sponsor and age group enrolled (supplemental Figure 1A) found that adult trials and those not sponsored by the NIH had significant increases in reporting according to race, but NIH-sponsored and pediatric trials did not.

Changes in Race and Race-Ethnicity Reporting Proportions Between 2005-2008 and 2011-2014. Dyadic bar chart of reporting proportions of race and race-ethnicity according to trial (A) and patient population (B) between the periods before (2005-2008; top bars) and after (2011-2014; bottom bars) implementation of the reporting requirements. Proportions are shown overall and for AML and ALL individually. Arrows indicate the direction of change between the periods, and asterisks denote significance below the level of P = .05 (two-sided z-test). R&E, race and ethnicity.
Changes in Race and Race-Ethnicity Reporting Proportions Between 2005-2008 and 2011-2014. Dyadic bar chart of reporting proportions of race and race-ethnicity according to trial (A) and patient population (B) between the periods before (2005-2008; top bars) and after (2011-2014; bottom bars) implementation of the reporting requirements. Proportions are shown overall and for AML and ALL individually. Arrows indicate the direction of change between the periods, and asterisks denote significance below the level of P = .05 (two-sided z-test). R&E, race and ethnicity.
The proportion of enrollees for which race and race-ethnicity were reported are shown in Figure 3B. Overall, reporting proportions according to population increased significantly between the periods (race, 51.7% to 72.7%; race-ethnicity, 39.5% to 45.4%; P < .001). Reporting of race increased for both AML and ALL (47.6% to 70.7% and 69.8% to 86.0%; P < .001), and race-ethnicity reporting increased for those with AML (32.8% to 47.3%; P < .001) but decreased for ALL (69.4% to 32.7%; P < .001). Significant increases in reporting of race and race-ethnicity were seen for all trial sponsor and age group subgroups (supplemental Figure 1B); the exception was ALL race-ethnicity reporting, which only increased among pediatric trials.
Table 2 shows the changes in enrollment within each racial-ethnic category between studies enrolling in periods before and after the policy changes, adjusted for changes in disease incidence and NH-White enrollment between the periods. Enrollment of both NH-Black and Hispanic patients was significantly lower in the period after implementation of the reporting requirements for both AML and ALL.
Discussion
In this analysis of clinical trial enrollment and reporting for AML and ALL in the United States, data absenteeism was substantial, especially among adult trials and those not sponsored by the NIH. For both AML and ALL clinical trials, NH-White patients were enrolled at significantly higher rates than other groups. Enrollment disparities were lower for trials sponsored by the NIH and for pediatric trials, although disparities were still seen for patients in these groups. Overall, there were some improvements in the public disclosure of enrollee demographic characteristics after the federal reporting requirements were instituted, which coincided with a decrease in the diversity of Black and Hispanic enrollees. These data suggest that demographic reporting and enrollment diversity for acute leukemia trials are inadequate, and that either enrollment diversity is worsening or greater data transparency is uncovering more substantial enrollment disparities.
Understanding data absenteeism and enrollment disparities in clinical trials is essential for these curable, resource-intensive malignancies with unique patterns of care and enrollment. A lack of diverse recruitment biases the trial results and limits their generalizability to underrepresented populations. Acute leukemia therapeutics also have mechanistic targets and pharmacodynamics that correlate with demography, such as higher rates of IDH2 mutation in Black persons with AML and reduced vincristine metabolism in NH-White persons.9,15,28,29 The translational knowledge gained through correlative studies skews drug development to most benefit those similar to the enrolled populations. Poor enrollment diversity also directly leads to care disparities, given that the best cancer care is arguably delivered through trial participation.5-7 As novel therapeutics become more costly and complex, diverse recruitment is also essential for some barriers to care delivery to be understood before approval. The consequences of this latter point have been seen in multiple myeloma, where significant racial and ethnic enrollment disparities were found among trials of novel therapies30 and were followed by disparities in treatment diffusion.31
After the initial federal efforts aimed at increasing enrollment diversity through public reporting requirements were instituted, reporting remained suboptimal but increased for some populations, and especially for adult trials and those not sponsored by the NIH. Interestingly, there was a concurrent decrease in enrollment diversity after the reporting requirements were instituted. As adult trials and those not sponsored by the NIH had more substantial enrollment disparities, these concomitant changes suggest there is either a real decline in diversity or, as more data are reported, the actual degree of enrollment disparities is greater than what the reported data show.
One recent analysis of ClinicalTrials.gov found that public reporting has become more frequent across multiple cancer types, with the reporting rate for trials increasing from 5.1% in 2007 to 39.1% in 2017,32 while another showed decreasing racial-ethnic enrollment diversity over a similar period.33 The data presented herein link these disparate findings more closely to suggest that increased data transparency may be driving these concurrent trends. Since the period included in our study, further changes in the ClinicalTrials.gov reporting environment have been made to further expand data reporting requirements.34 Although the latency of acute leukemia incidence data are such that the consequences of these changes cannot yet be assessed, a reevaluation of public reporting after these updates, and their associations with enrollment diversity, should be performed once data sources are mature.
These enrollment diversity data support the growing evidence that cancer clinical trial enrollment disparities have overlapping etiologies, including disparate trial access, research mistrust, increased trial participation costs, and unnecessarily restrictive enrollment criteria, which a single intervention cannot resolve.4,6,7,35 The particularities of acute leukemia care mean that overcoming enrollment disparities will likely require multilevel interventions that are specific to AML and ALL.3,7,36 Although reporting and disclosure represent a key behavioral intervention in medicine, that of performance feedback,10 successful change using this mechanism requires reporting to be directed at individuals, given in a timely manner, and provided alongside recommendations for how to improve. Feedback is adaptable for use at multiple levels, but available data show that a reporting feedback intervention attempting to increase enrollee diversity should be directed at individual providers at a site or recruiting to a trial to have the highest chance of success. Indeed, greater data transparency is the foundation upon which disparities interventions must be built. Without it, data absenteeism and data chauvinism8 will continue to overfit trial results to the outcomes of NH-White subjects. Feedback interventions, such as multilevel real-time enrollment reports, are an intriguing mechanism that may yet bolster disclosure and diversity, but they should be designed according to best practices and through community involvement.
Our work has limitations. First, these data are observational and aggregate in nature and cannot account for other social or environmental determinants of health that may mediate the disparities seen. Our data also rely on accurate enrollment reporting to ClinicalTrials.gov. Although we tried to ensure their accuracy by reviewing the ClinicalTrials.gov reports of results against publications and through study contacts, these data remain a proxy source and subject to investigators correctly inputting them into the database. Second, we limited our inclusion to studies within the United States, but these data do not differentiate between patients from within or outside the United States who were recruited at US sites. Third, while annualized SEER data were used to calculate incidence, decennial census data were static, and racial-ethnic subgroup migration into or out of the registry areas over time may have changed actual population proportions. Fourth, the amount of unreported enrollment data are both a limitation of this work and an important finding. Characterizing data absenteeism is crucial to fostering transparency, and the bias of unreported data are more likely to underestimate disparities than overreport them.8 Finally, these data cannot directly suggest how to increase enrollment diversity, only that disparities exist for the acute leukemias and that the demographic reporting requirements implemented were not successful at significantly improving trial diversity.
As future acute leukemia clinical trials are planned, expanded enrollment sites, eligibility criteria, and culturally competent enrollment methods must be enacted to increase participant diversity. Further innovations are sorely needed to connect patients to appropriate clinical trials and to overcome structural and clinician-based recruitment barriers; examples include creating multilevel enrollment reporting feedback interventions, designing expansion cohorts specifically for underrepresented groups, and developing ethical reimbursement strategies for participation. A crucial first step is to ensure that demographic enrollment data are publicly reported, and data absenteeism and chauvinism are overcome.
Acknowledgments
This work was supported by grants from the NIH, National Cancer Institute (T32 CA092203 and P50 CA206963, A.H).
The sponsors of this study are public or nonprofit organizations that support science in general. They had no role in gathering, analyzing, or interpreting the data. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the US government.
Authorship
Contribution: A.H., D.J.D., and G.A.A. designed the research; A.H. abstracted the data; A.H. and G.A.A. performed the analysis; M.R.L., J.S.G., W.S., and D.J.D. provided critical analytic review; A.H. wrote the manuscript; and M.R.L., J.S.G., W.S., D.J.D., and G.A.A. provided critical review of the manuscript.
Conflict-of-interest disclosure: J.S.G. receives research funding from AbbVie, Genentech, Pfizer, Prelude, AstraZeneca, and Lily; and has a consultancy/advisory role for AbbVie and Takeda. W.S. receives honoraria from UpToDate and Research To Practice; speaker honoraria from AbbVie and Pfizer; and has a consultancy/advisory role for Servier, Kite, Pfizer, Daiichi, Astellas, and Agios. D.J.D. has a consultancy/advisory role for AbbVie, Amgen, Agios, Autolus, Blueprint, Forty-Seven, GlycoMimetics, Incyte, Jazz, Kite, Novartis, Pfizer, Servier, and Takeda; and receives research funding from AbbVie, Novartis, Blueprint, and GlycoMimetics. The remaining authors declare no competing financial interests.
Correspondence: Gregory A. Abel, Dana-Farber Cancer Institute, 450 Brookline Ave, Boston, MA 02215; e-mail: gregory_abel@dfci.harvard.edu.