

Key Points
Eight cycles of KRd as induction/consolidation, plus transplant, is highly effective in newly diagnosed multiple myeloma.
Responses are rapid and deep with improvement at each step up to a clonal level.

Abstract
Bortezomib, lenalidomide, and dexamethasone plus transplant is a standard of care for eligible patients with multiple myeloma. Because responses can deepen with time, regimens with longer and more potent induction/consolidation phases are needed. In this phase 2 study, patients received eight 28-day cycles of carfilzomib (K) 20/36 mg/m2 (days 1-2, 8-9, 15-16), lenalidomide (R) 25 mg (days 1–21), and dexamethasone (d) 20 mg (days 1-2, 8-9, 15-16, 22-23). All patients proceeded to transplant after 4 cycles and received 1 year of lenalidomide maintenance (10 mg, days 1-21). The primary objective was stringent complete response at the completion of consolidation. Overall, 48 patients were screened and 46 enrolled; 21% had adverse cytogenetics. Among 42 evaluable patients after consolidation, 26 were in stringent complete response (CR; 61.9%), 27 were at least in CR (64.3%): 92.6% had undetectable minimal residual disease according to flow cytometry (≥2.5 × 10−5) and 63.0% according to next-generation sequencing (10−6). Median time to CR was 10.6 months. According to multiparametric flow cytometry and next-generation sequencing, 69.0% and 66.7% of patients, respectively, had undetectable minimal residual disease at some point. With a median follow-up of 60.5 months, 21 patients progressed, and 10 died (7 of multiple myeloma). Median progression-free survival was 56.4 months. There were no KRd-related deaths. Four patients discontinued the program due to toxicities; 56 serious adverse events were reported in 31 patients, including 8 cardiovascular events (2 heart failures, 5 pulmonary embolisms or deep vein thrombosis). Common grade 3/4 adverse events were hematologic (74%) and infectious (22%). In summary, 8 cycles of KRd produce fast and deep responses in transplant-eligible patients with newly diagnosed multiple myeloma. The safety profile is acceptable, but cardiovascular adverse events should be closely monitored. This clinical trial is registered at www.clinicaltrials.gov as #NCT02405364.
Introduction
Front-line therapy in symptomatic patients with newly diagnosed multiple myeloma (NDMM) has been highly modified during the last decades, but high-dose therapy with autologous stem cell transplantation (ASCT) is still a standard of care for eligible patients.1 Combination therapy with proteasome inhibitors and immunomodulatory drugs has expanded treatment options and improved response rates and survival outcomes. Data published using thalidomide or lenalidomide, plus bortezomib and dexamethasone (RVd)1-11 in the transplant setting, have established them as standards of care in patients with NDMM. Since then, many groups have attempted to build on the success with these regimens. These efforts include prolonging induction and/or consolidation phases and extended use of lenalidomide instead of thalidomide. The Spanish group11 proposed 6 cycles of RVd induction, but the benefit of bortezomib could be hampered over time by drug-induced neurologic side effects, leading to dose reductions, impairment of quality of life, and treatment discontinuation. This scenario could be particularly true with prolonged induction and/or consolidation.
Carfilzomib is a second-generation, non-neurotoxic, proteasome inhibitor approved in patients with relapsed/refractory MM in combination with Rd. Carfilzomib has shown promising results on safety and efficacy in a phase 1/2 trial in patients with NDMM.12 We therefore hypothesized that switching from bortezomib to carfilzomib (K) could improve the stringent complete response (sCR) rate without increasing toxicities. In this phase 2 trial, the Intergroupe Francophone du Myélome assessed the efficacy and safety of a total of 8 cycles of KRd as induction (4 cycles) and consolidation (4 cycles) in transplant-eligible patients with NDMM, followed by 1 year of lenalidomide maintenance.
Materials and methods
Patients
Patients aged <66 years with symptomatic and measurable disease were included in this trial provided they had not received any previous myeloma therapy and were eligible for transplant. The exclusion criteria included: creatinine clearance <50 mL/min; a serum total bilirubin concentration >2.0 mg/dL; serum aspartate/alanine aminotransferase levels or alkaline phosphatase levels >3.5 times the upper limit of the normal range; history of unstable angina or myocardial infarction within 6 months before enrollment, New York Heart Association functional class III or IV heart failure, uncontrolled angina, history of severe coronary artery disease, severe uncontrolled ventricular arrhythmias, and grade 3 conduction system abnormalities unless the subject has a pacemaker; uncontrolled hypertension or uncontrolled diabetes; significant neuropathy (grades 3/4, or grade 2 with pain); contraindication to anticoagulant prophylaxis; and history of any other malignant disease with the exception of basal cell carcinoma and stage I cervical cancer.
The institutional ethics committees approved the study, which was conducted according to the Declaration of Helsinki and the International Conference on Harmonisation guidelines. All patients provided written informed consent before entering the study. This clinical trial is registered at www.clinicaltrials.gov as #NCT02405364.
Study design and treatment
This multicenter, single-arm, open-label, phase 2 study was conducted at 10 centers in France, with enrollment between March and November 2014. Treatment comprised four 28-day cycles of intravenous carfilzomib (20-36 mg/m2) on days 1 to 2, 8 to 9, 15, and 16; oral lenalidomide (25 mg) on days 1 to 21; and oral dexamethasone (20 mg) on days 1 to 2, 8 to 9, 15 to 16, 22, and 23. Stem cell harvest was planned for all patients after high-dose cyclophosphamide (3 g/m2) plus granulocyte colony-stimulating factor (5 µg/kg according to local practice) with a goal of at least 5 × 106 CD34 cells/kg for 2 potential ASCTs (with a minimum required of 2 × 106 CD34/kg for 1 ASCT). Patients proceeded to a single transplant using melphalan 200 mg/m2 as conditioning. Two months after hematologic recovery, patients without disease progression could receive consolidation therapy with four 28-day KRd cycles, using the same schedule as induction, at the last tolerated dose for carfilzomib and lenalidomide, with weekly dexamethasone (20 mg). Patients subsequently received maintenance therapy with oral lenalidomide (10 mg/d, days 1-21 of 28-day cycles) for 1 year (13 cycles). Dose reductions for treatment-related toxicities were as follows: carfilzomib from 36 mg/m2 to 27 mg/m2 to 20 mg/m2 to 15 mg/m2 to 11 mg/m2; lenalidomide from 25 mg/d to 20 mg to 15 mg to 10 mg to 5 mg, and dexamethasone from 20 mg/d twice weekly to 20 mg weekly to 20 mg every other week. Unless contraindicated, all patients received anticoagulation for prevention of deep-vein thrombosis with low-molecular-weight heparin, antiviral therapy for herpes zoster prevention, and antibiotic prophylaxis for bacterial infections until completion of all therapy.
Assessment of efficacy and safety
The primary end point was the sCR rate at the completion of consolidation. Secondary end points included response at each step of the treatment program, time to response, quality of stem cell collection, progression-free survival (PFS), overall survival (OS), and safety. Myeloma response assessment was based on modified International Myeloma Working Group uniform response criteria.13 CR was defined as negative serum and urine immunofixation, absence of soft tissue plasmacytoma, normal calcium concentration, and <5% plasma cells in bone marrow. sCR was defined with the these criteria plus a normal free light chain ratio. Minimal residual disease (MRD) was assessed by multiparametric flow cytometry (MFC) of plasma cells at a sensitivity at least 2.5 × 10−5 (Soraya Wuilleme and Nelly Robillard, Central Laboratory of Hematology, University Hospital of Nantes, Nantes, France) at each step of the program for patients at least in very good partial response (VGPR). For informative and evaluable patients, MRD was also assessed by using next-generation sequencing (NGS) at a sensitivity at 10−6 (Hervé Avet-Loiseau and Jill Corre, Laboratory for Genomics in Myeloma, Toulouse, France).
All patients were followed up until death or end of the study (November 2019). Safety was monitored until 30 days after the last dose of study drug, and all along during follow-up for secondary malignancies. Toxicities were graded according to National Cancer Institute Common Toxicity Criteria of Adverse Events version 4.03 (Bethesda, MD).
MRD evaluation by MFC
MRD was evaluated for patients in VGPR or better at the following time points: postinduction/pretransplant, posttransplant, postconsolidation, 6-month maintenance, and postmaintenance. The samples were processed after red blood cell lysis (VersaLyse, Beckman Coulter, Brea, CA) and phosphate-buffered saline washing. Surface antigens and cytoplasmic immunoglobulin light chain staining was then performed after IntraStain (Dako, Glostrup, Denmark) cell permeabilization. We used a 7-color combination of fluorescein isothiocyanate conjugated anti-λ light chains (BD Biosciences, San Jose, CA), phycoerythrin-conjugated CD28 and CD56 (BD Biosciences), PC5-conjugated CD138 (Beckman Coulter, Miami, FL), phycoerythrin/Cy7-conjugated CD19 (Beckman Coulter), allophycocyanin (APC)-conjugated anti-κ light chains (BD Biosciences), APC-H7–conjugated CD45 (BD Biosciences), and HorizonV450-conjugated CD38 (BD Biosciences).14 Data were acquired on an FACSCanto II flow cytometer equipped with FACSDiva version 6.2 data acquisition and analysis software (BD Biosciences), and the analysis of all plasma cell subsets was performed as reported. All events of each tube were acquired. To detect MRD at a sensitivity of at least 2.5 × 10−5, the minimum number of total nucleated cells required was 2 × 106 with a minimum neoplastic population size of 20 events.15
MRD evaluation by NGS
Collected bone marrow samples were frozen as dry pellets and stored at −80°C until analysis. The technique is based on the sequencing of immunoglobulin genes, which are clonally rearranged in all patients with MM and thus represent unique, patient-specific biomarkers. The clonal rearrangements were identified by using the NGS commercial kit for MRD assay (Adaptive Biotechnologies, San Francisco, CA). For MRD quantification, DNA was extracted from the bone marrow samples and amplified by polymerase chain reaction using immunoglobulin gene-specific primers; the amplified products were then sequenced. The sensitivity was 10−6, meaning that patients were considered MRD undetectable when the level was below 10−6. Patients who failed to achieve at least a VGPR, who were not evaluated, or who did not enter the maintenance phase of the trial were considered as having persistent MRD.
Statistical methods
The sCR rate at the completion of consolidation, based on investigator assessment and reviewed by a medical monitor, was the primary end point for the sample size calculation. A sample size of 42 patients was required to decide whether the proportion of patients achieving an sCR could be increased from the expected level of 40% after consolidation to 60%. With 5% type I error and 80% power, a total of 23 or more sCRs were required to claim activity of the transplant program with the KRd regimen as induction and consolidation.16 To take into account a 10% risk of dropoff, 46 patients were included. The efficacy population comprised all patients who received at least 1 dose of study treatment and who had either a response that could be evaluated at completion of consolidation therapy or who had had progressive disease before this time. The treated population comprised all patients who received at least one dose of study treatment. An exact binomial test was used for testing our hypothesis on the efficacy population. We also performed a sensitivity analysis that included all treated patients considering that patients have failed to reach sCR if they stopped treatment before post-consolidation assessment, regardless of their response. The MRD rate was estimated for evaluable population, and patients in partial response (PR) or less were scored positive.
Median follow-up duration was estimated by using the reverse Kaplan-Meier method. PFS was calculated as the time from start of treatment to the first documentation of progressive disease, or death if the patient died due to any cause before progression. OS was calculated as the time from the start of treatment to death. The Kaplan-Meier method was used to estimate the survival distribution. For survival analysis, patients’ MRD status (according to MFC) was analyzed as a time-varying variable. All analyses were conducted by using SAS (Statistics Solutions).
Results
Patients’ disposition and characteristics
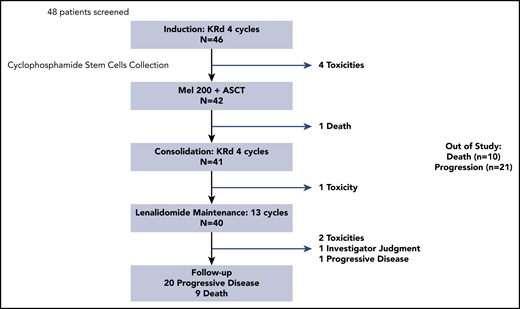
Forty-eight patients with symptomatic NDMM were screened; 46 were enrolled and received at least 1 dose of treatment during the induction phase. Reason for screen failure was renal dysfunction in 2 patients. Overall, 46 patients received induction, 43 patients underwent mobilization (3 patients were withdrawn from treatment due to toxicities), and 42 underwent transplantation (1 patient had progressive disease), 41 entered the consolidation phase (1 patient died after transplant), and 40 entered the maintenance phase (1 patient was withdrawn from treatment due to toxicity) (Figure 1). Baseline demographic and disease characteristics are summarized in Table 1. The median age at start of therapy was 56 years (range, 40-65 years). Fluorescence in situ hybridization analysis was informative in 43 patients (93.5%), including the presence of a chromosome 17p deletion (with a positive 50% cutoff) in 4 patients (9.3%) and t(4;14) in 5 patients (11.6%). Overall, 9 patients (20.9%) were classified as high-risk MM with del17p or t(4;14).
Baseline demographic and disease-related characteristics of patients (N = 46)
| Characteristic | Value |
|---|---|
| Sex, N | |
| Male | 32 |
| Female | 14 |
| Median age, y (IQR) | 56 (50-62) |
| ECOG, N (%) | |
| 0 | 23 (51) |
| 1 | 18 (40) |
| 2 | 4 (9) |
| Isotype, n (%) | |
| Immunoglobulin G | 31 (67.5) |
| Immunoglobulin A | 8 (17.5) |
| Light chain | 5 (11) |
| Other | 2 (4) |
| ISS stage, N (%) | |
| I | 21 (46) |
| II | 22 (48) |
| III | 3 (6) |
| Median bone marrow plasma cells, % (IQR) | 19.5 (12.0-30.5) |
| Median creatinine, µmol/L (IQR) | 80 (65-91) |
| Median calcium, mmol/L (IQR) | 2.28 (2.21-2.39) |
| Median β2-microglobulin, mg/L (IQR) | 2.85 (2.12–3.47) |
| Median albumin, g/L (IQR) | 35.6 (31.8-41.6) |
| FISH analysis, N (%) | 43 evaluable/46 |
| del(17p) with a 50% positive cutoff, | 4 (9.5) |
| t (4;14), | 5 (11.5) |
| Characteristic | Value |
|---|---|
| Sex, N | |
| Male | 32 |
| Female | 14 |
| Median age, y (IQR) | 56 (50-62) |
| ECOG, N (%) | |
| 0 | 23 (51) |
| 1 | 18 (40) |
| 2 | 4 (9) |
| Isotype, n (%) | |
| Immunoglobulin G | 31 (67.5) |
| Immunoglobulin A | 8 (17.5) |
| Light chain | 5 (11) |
| Other | 2 (4) |
| ISS stage, N (%) | |
| I | 21 (46) |
| II | 22 (48) |
| III | 3 (6) |
| Median bone marrow plasma cells, % (IQR) | 19.5 (12.0-30.5) |
| Median creatinine, µmol/L (IQR) | 80 (65-91) |
| Median calcium, mmol/L (IQR) | 2.28 (2.21-2.39) |
| Median β2-microglobulin, mg/L (IQR) | 2.85 (2.12–3.47) |
| Median albumin, g/L (IQR) | 35.6 (31.8-41.6) |
| FISH analysis, N (%) | 43 evaluable/46 |
| del(17p) with a 50% positive cutoff, | 4 (9.5) |
| t (4;14), | 5 (11.5) |
ECOG, Eastern Cooperative Oncology Group; FISH, fluorescence in situ hybridization; ISS, International Staging System.
Response assessments
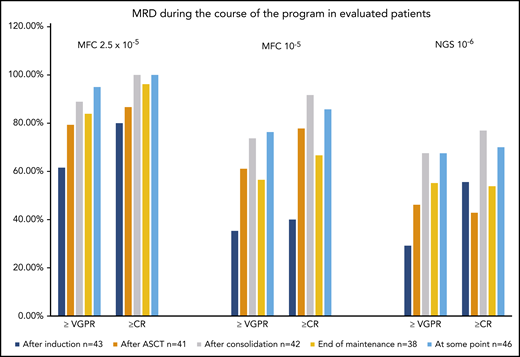
At the completion of consolidation therapy, 26 (61.9%) of 42 patients reached sCR (90% CI, 48.0-74.4; P = .0034). According to the sensitivity analysis of the primary end point, the sCR rate was 56.5% (90% CI, 43.4-69.0; P = .0172). Twenty-seven (64.3%) patients were at least in CR, and 25 (92.6%) patients were MRD-undetectable according to MFC (2.5 × 10−5) and 17 (63.0%) according to NGS (10−6). The proportion of VGPR or better was 92.9%, and the overall response rate was 97.7%. Figures 2 to 3 show the response rates at different time points plus MRD according to MFC and NGS. The median time to PR and CR was 0.95 (not estimable) and 10.6 (7.9-13.4 excluded) months, respectively. Responses deepened at all stages throughout the program. Overall, transplant improved responses in 9 patients and KRd consolidation in 13 patients. Seven patients had further response improvement with 1 year of lenalidomide maintenance. Proportions of patients with at least PR, VGPR, and CR as best responses during the study were 46 (100%), 43 (93.5%), and 34 (73.9%). Overall, 38 (90.5%) patients had undetectable MRD by MFC (2.5 × 10−5), 29 (69.0%) patients by MFC at 10−5, and 28 (66.7%) by NGS (10−6) at some point.
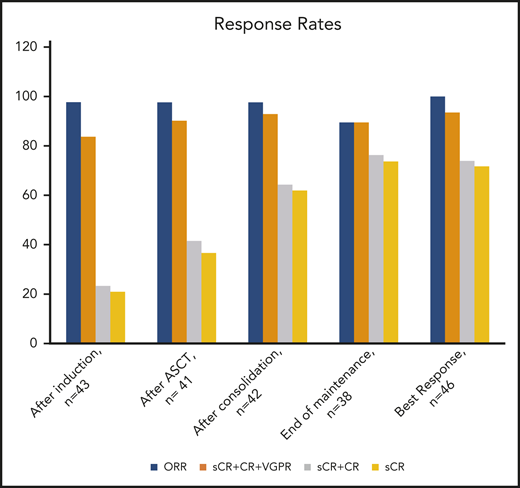
Summary of responses in the evaluable treated population. ORR, overall response rate.
Summary of responses in the evaluable treated population. ORR, overall response rate.
Survival outcomes
As of November 2019, the median follow-up from start of therapy was 60.5 months (58.7-62.1 months). Twenty-one patients had disease progression, and 10 died (3 did not progress). The median PFS was 56.4 months (95% CI, 43.5 to not evaluable), and the median OS was not reached. Estimated 5-year PFS and OS were 45.1% (95% CI, 26.9-59.4) and 77.8% (95% CI, 62.7-87.4), respectively (Figure 4). The median PFS was 43.5 months in patients who were MRD-persistent (MFC sensitivity 10−5) vs not reached in patients who were MRD-undetectable (Figure 5).
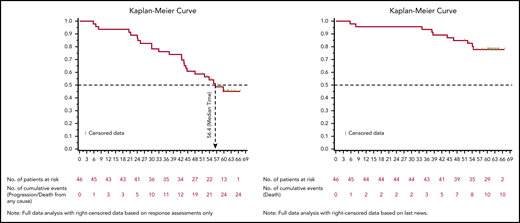
Kaplan-Meier curves showing survival numbers from the first study treatment population. PFS (A) and OS (B) (full data analysis with right-censored data based on response assessments).
Kaplan-Meier curves showing survival numbers from the first study treatment population. PFS (A) and OS (B) (full data analysis with right-censored data based on response assessments).
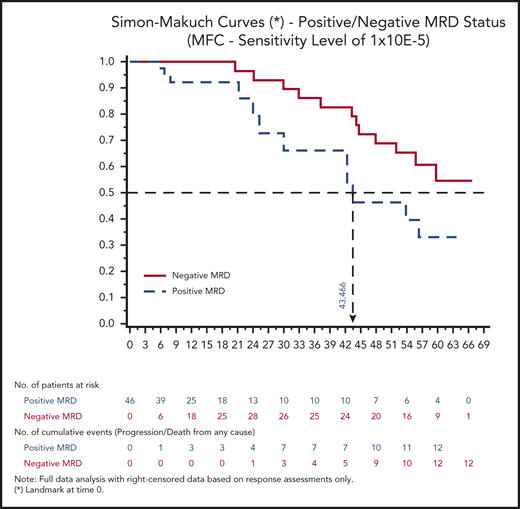
PFS for positive/negative MRD status (MFC sensitivity level of 10−5) from first study treatment administration. Simon-Makuch curves in the treated population (full data analysis with right-censored data based on response assessments).
PFS for positive/negative MRD status (MFC sensitivity level of 10−5) from first study treatment administration. Simon-Makuch curves in the treated population (full data analysis with right-censored data based on response assessments).
Stem cell harvesting and transplantation
Forty-three patients successfully underwent stem cell collection with a median of 7.88 × 106 CD34+ cells/kg (interquartile range [IQR], 6.35-11.38 × 106) harvested. After cyclophosphamide mobilization, 8 (18.6%) patients failed to reach the target of 5 × 106 CD34 cells per kg and required plerixafor. No patient experienced stem cell collection failure. All but 4 patients underwent high-dose therapy as scheduled in the program, with no engraftment delay or unexpected complications. The median time to neutrophils recovery (≥500/mm3) and platelets recovery (≥20 g/L) was 13 days (IQR, 12;14) and 12 days (IQR, 11;13), respectively.
Treatment exposure and safety
There were no KRd-related deaths. Overall, 4 patients (8.7%) permanently discontinued combined treatment due to serious adverse events (SAEs): 3 (6.5%) during induction (1 heart failure, 1 pneumonia, 1 jugular vein thrombosis) and 1 posttransplant (fatal septic shock). Eleven (23.9%) patients had AEs leading to permanent discontinuation of at least one study drug. Seven (15.2%) patients permanently discontinued carfilzomib because of cardiac failure (n = 2), neutropenia (n = 2), extensive jugular thrombosis (n = 1), pneumonia (n = 1), and clinical intolerance (n = 1). Seven (15.2%) patients stopped lenalidomide, and 6 (13%) stopped dexamethasone. During KRd induction and consolidation, at least 1 dose modification was required in 28 (60.9%) patients. This included 23 (50.0%), 20 (43.5%), and 17 (37.0%) patients who required carfilzomib, lenalidomide, and dexamethasone dose modifications, respectively. Concerning carfilzomib, reasons for modifications were pneumonia (n = 3), liver disorders (n = 2), fever (n = 2), flu-like symptoms (n = 2), gastrointestinal tract symptoms, neutropenia, skin disorders, herpes zoster, thrombocytopenia, bradycardia, bronchitis, pulmonary embolism, hyperglycemia, neuropathy, and cramps. During maintenance, 23 (57.5%) of 40 patients received 13 cycles (1 complete year) of lenalidomide at the planned full dose (10 mg). The dropout rate of lenalidomide was 12% (grade 3/4 neutropenia, rash, or relapsed disease) and 1 patient stopped maintenance therapy before 6 months. Overall, 10 (25%) of 40 patients had at least 1 dose modification.
With respect to safety data, 56 SAEs were reported in 31 patients (67.4%), including 23 treatment-emergent SAEs in 19 patients (41.3%): 4 patients with cardiac disorders (2 heart failures, 1 bradycardia, and 1 intracardiac thrombus), 4 patients with vascular disorder (2 pulmonary embolisms and 2 deep vein thrombosis), febrile neutropenia (n = 3), and second primary neoplasm (n = 5). Other SAEs included infections in 12 patients (26.1%) and musculoskeletal disorders in 9 patients (19.6%). Grade 3/4 toxicities during the program, excluding stem cell harvest and transplant, are shown in Figure 6. At least one grade 3/4 treatment-emergent AE was reported in 45 patients (97.8%). The most common grade 3/4 treatment-emergent AEs were hematologic toxicities (induction, 26.1%; consolidation, 75.6%) and infections (induction, 19.6%; consolidation, 2.4%).
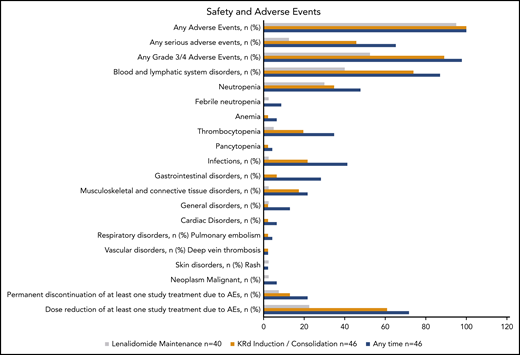
AEs in the treated population (N = 46) at any time and during KRd induction/consolidation or lenalidomide maintenance.
AEs in the treated population (N = 46) at any time and during KRd induction/consolidation or lenalidomide maintenance.
Grade 3/4 hematologic toxicities included lymphopenia (65.2%), neutropenia (34.8%), thrombocytopenia (19.6%), and anemia (2.2%). During lenalidomide maintenance therapy, predominant grade 3/4 toxicities were also hematologic (40.0%), with grade 3/4 neutropenia (30.0%), lymphopenia (10.0%), and thrombocytopenia (5.0%). Only 1 patient had febrile neutropenia. Overall, 20 patients had cardiovascular disorders: 2 heart failures, 6 cardiac rhythm disorders, 7 high blood pressure, and 13 venous thromboembolic events with 2 pulmonary embolisms, 1 extensive jugular thrombosis, 6 superficial thrombosis, and 1 intracardiac thrombus. All except 3 resolved without sequelae. No patient experienced grade 3/4 peripheral neuropathy events or grade 2 or worse neuralgia. Grade 1/2 sensory peripheral neuropathy was reported in 13 (28.3%) patients. During follow-up, 5 patients (10.9%) had a second primary malignancy, including 1 AML (2.2%) and 4 (8.7%) solid tumors.
Discussion
The primary objective of this trial was to explore the efficacy of a transplant program in NDMM patients with extended KRd induction and consolidation (8 cycles). Here we report both rapid and deep responses. At the completion of consolidation, 62% of patients reached sCR, with 64% of patients in confirmed CR. Our study showed that depth of responses continuously increased throughout the program. Rates of CR or better upgraded from 23% after induction to 41.5% after transplant and 64.5% at the completion of consolidation. Fixed 1-year lenalidomide maintenance further deepened responses in 7 patients (18%).
Improvement of PFS and OS are the primary goals of treatment for patients with MM. Several groups reported that survival is correlated to a deep and sustained response, and undetectable MRD by MFC (10−5) is an established major prognostic factor for clinical outcomes.17-19 In our previous large phase 3 trial of RVd, MRD was undetectable (MFC sensitivity 10−4) during the study in 79% of the patients in the transplant arm.1 In the current trial, we were able to evaluable MRD according to MFC at a sensitivity of at least 2.5 × 10−5 for all patients and according to NGS with a sensitivity of 10−6 for >80% of patients. Using this program with 8 cycles of KRd plus transplant, 69.0% of patients achieved undetectable MRD according to MFC (10−5) and almost 67.0% by NGS (10−6). If we consider only patients who are CR or better, 25 of 27 patients were MRD-undetectable by MFC (2.5 × 10−5) and 17 of 27 by NGS (10−6) at the completion of consolidation. Of note, 21 (63.6%) patients achieved 1-year sustained undetectable MRD by MFC from start of maintenance, and 5 became undetectable during maintenance.
Clinical outcomes are promising, with an estimated 5-year OS of 77.8% and a median PFS of 56.4 months. Interestingly, the median PFS was not reached for patients who were MRD-undetectable vs 43.5 months for patients who were MRD-persistent (MFC 10−5). At the end of study, 22 patients are alive and progression-free, of whom 16 had undetectable MRD by NGS at some point. These results compare favorably with the updated data recently published by the Multiple Myeloma Research Consortium (MMRC)20 with a similar induction and transplant program but a longer consolidation (12 KRd cycles and prolonged lenalidomide maintenance): 65% of patients achieved CR or better at the completion of consolidation (12 KRd cycles) and a 70% undetectable MRD rate according to NGS (10−5). With a median follow-up of 56 months, the 5-year PFS and OS were 72% and 84%, respectively. MRD-negative patients had an estimated 85% 5-year PFS. All together, these data strongly suggest that undetectable MRD could be the goal of treatment in front-line MM transplant-eligible patients and a surrogate marker for survival outcome.21 Because MRD is part of the International Myeloma Working Group response criteria13 for patients achieving CR, it could be the primary end point for phase 3 trials. MRD monitoring may also be used to tailor therapy in MM. To do so, the MRD techniques need to be sensitive, broadly applicable, reliable, and affordable. Both MFC and NGS can achieve the 10−5 sensitivity required for MRD determination. However, these methods are not interchangeable, and the discrepancies observed between them require consistency in the methodology used for measurement.
Future studies will also be required to determine the impact of MRD sustainability on prognosis and standardization of this definition. Actually, recent data from the large phase 3 FORTE trial22 (including 4 cycles of KRd induction, followed by transplant, and 4 cycles of KRd consolidation, n = 158; or 12 cycles of KRd without transplant, n = 157) validate that KRd induction and consolidation can give rapid and deep response rates with >54% of patients achieving an undetectable MRD by MFC (10−5). Among patients who achieved CR or better in the KRd transplant arm, 83% were MRD undetectable according to MFC (at least 10−5) and 34% according to NGS (10−6),23 but one should consider that not all CR patients were evaluable at a sensitivity level of 10−6. The FORTE study also confirms the major role of transplant in maintaining undetectable MRD and further prolonging PFS: 68% of patients in the KRd transplant arm had 1-year sustained undetectable MRD vs 54% in the nontransplant arm.22 With a median follow-up of 45 months, the estimated 3-year PFS is 83% for NGS MRD-undetectable patients, with a 94% rate of 1-year sustained MRD negativity.24 In the current study, the 1-year sustained MRD negativity rate after consolidation was 63.6% according to MFC (2.5 × 10−5) (55% for the MMRC with continuous postconsolidation therapy). Concerning high-risk patients (n = 9 of 46) in the current trial, all except 2 achieved at least CR at the completion of consolidation and reached undetectable MRD according to NGS. Data on patients with t(14;16) or 1q gain are not available. During follow-up, all but one relapsed, and these data could favor the role of long-term therapy for high-risk patients. This concept is supported with data from the MMRC study in which maintenance was continued until progression and where high-risk patients (n = 27 of 76) had an estimated 5-year PFS of 57% that reached 77% if MRD was undetectable according to NGS (10−5).20
An important objective of this phase 2 trial was also to evaluate the safety of our extended KRd transplant program. As anticipated, the strategy was feasible (87% completed the planned sequence) with no KRd-related mortality. Overall, 33 (72%) patients had at least 1 dose modification in any of the study drugs: 17 during induction and 17 during consolidation. The hematologic toxicities were predictable and manageable. Grade 3/4 lymphopenia, neutropenia, and thrombocytopenia most of the time occurred during consolidation. Considering nonhematologic toxicities, grade 3/4 infectious disorders (bronchitis and pneumonia) were likely reported during the induction phase. The main concerns with the KRd regimen were cardiovascular events, with 8 SAEs reported (cardiac failure, n = 2; bradycardia, n = 1; thromboembolic events, n = 5). Considering all grades of AEs, 13 patients had deep and superficial venous thromboembolic events despite prophylaxis, 5 had cardiac rhythm disorders, and 7 had hypertension during induction or consolidation. The thromboembolic events could be explained by the choice of the low-molecular-weight heparin product and underlying conditions (ie, obesity, hemoglobinopathy, diabetes). Only 1 grade 3/4 acute kidney injury was reported. Overall, these toxicities related to carfilzomib and lenalidomide were mostly manageable and reversible, but 4 patients did not proceed to transplant and discontinued the program. Indeed, meta-analysis of treatment-emergent AEs with carfilzomib25 and safety data from the FORTE trial highlight that cardiovascular events must be closely monitored, especially thrombosis and high blood pressure, to avoid these side effects.26,27 Patients should be accurately evaluated at diagnosis by using echocardiography and closely monitored to mitigate heart failure and hypertension. Appropriate antithrombotic prophylaxis is also mandatory.
In summary, a transplant-based regimen built around carfilzomib, lenalidomide, and dexamethasone as induction and consolidation, followed by 1 year of lenalidomide maintenance, is highly effective in patients with NDMM. Responses are rapid and deep, with improvement at each step, including deepening rates of undetectable MRD. These results are comparable to the original KRd studies from Jakubowiak et al12,20,28 and the data from Landgren et al.29 The safety profile is acceptable, especially if patients undergo regular, close monitoring to minimize cardiovascular and thrombotic toxicities. Cross-trial comparisons favor KRd as a modern induction and consolidation regimen. Conflicting data was recently reported from the phase 3 Eastern Cooperative Oncology Group ENDURANCE (Bortezomib or Carfilzomib With Lenalidomide and Dexamethasone in Treating Patients With Newly Diagnosed Multiple Myeloma) trial30 (no superiority of KRd regimen vs bortezomib, lenalidomide, and dexamethasone in standard or intermediate-risk NDMM patients without transplant); however, the promising results of the ongoing randomized large phase 3 studies with transplant arms (the FORTE study and UK NCRI Myeloma XI intensive group)31 will help validate the KRd approach in the transplant setting. Other studies also showed that KRd represents a potent choice as a backbone for quadruplet therapy along with the anti-CD38 monoclonal antibody for NDMM (daratumumab-KRd,32 isatuximab-KRd33 ). After approval of the 4-drug combination daratumumab + bortezomib-thalidomide-dexamethasone,34 the KRd regimen plus anti-CD38 monoclonal antibody therapy will be the future platform of our MRD-driven studies in transplant-eligible patients with NDMM.
Presented in oral abstract form at the 58th Annual Meeting of the American Society of Hematology. 5 December 2016. San Diego, CA.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
For original data, e-mail the corresponding author.
There is a Blood Commentary on this article in this issue.
Acknowledgments
The authors gratefully acknowledge the work performed by individual research teams at all participating study sites. They are also indebted to Laure Devlamynck for biostatistical analyses, Christopher Venner and Simon Gibbs for their critical reading of the manuscript, Claire Mathiot, Catherine Boccaccio, Chantal Nobili-Escriva, and Amandine Huguet for their administrative and material support, and Cathy Payen for the medical monitoring.
This trial was supported by research funding and drug supply from Amgen and Celgene.
Authorship
Contribution: M.A., V.L.-C., and M.R. designed the research and analyzed the data; M.A., V.L.-C., M.R., S.W., and J.C. wrote the paper; and all authors reviewed and agreed on the final version as submitted.
Conflict-of-interest disclosure: M.R., K.B., S.M., L.G., L.B., D.C., C.S., C.T., P.M., X.L., T.F., J.D., B.H., J.C., and M.A. have participated in lectures for Amgen and/or Celgene. The remaining authors declare no competing financial interests.
Correspondence: Murielle Roussel, Service d’Hématologie, IUC Oncopole, 1 Avenue Irène Joliot Curie, 31059 Toulouse Cedex 9, France; e-mail: roussel.murielle@iuct-oncopole.fr.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal