

Key Points
In patients with newly diagnosed mIDH1 AML (median age, 76 years), ivosidenib monotherapy achieved median overall survival of 12.6 months.
The CR/CRh rate was 42.4%; mutation clearance in 64% patients with CR/CRh suggests that ivosidenib alters the biology of mIDH1 AML.

Abstract
Ivosidenib (AG-120) is an oral, targeted agent that suppresses production of the oncometabolite 2-hydroxyglutarate via inhibition of the mutant isocitrate dehydrogenase 1 (IDH1; mIDH1) enzyme. From a phase 1 study of 258 patients with IDH1-mutant hematologic malignancies, we report results for 34 patients with newly diagnosed acute myeloid leukemia (AML) ineligible for standard therapy who received 500 mg ivosidenib daily. Median age was 76.5 years, 26 patients (76%) had secondary AML, and 16 (47%) had received ≥1 hypomethylating agent for an antecedent hematologic disorder. The most common all-grade adverse events were diarrhea (n = 18; 53%), fatigue (n = 16; 47%), nausea (n = 13; 38%), and decreased appetite (n = 12; 35%). Differentiation syndrome was reported in 6 patients (18%) (grade ≥3 in 3 [9%]) and did not require treatment discontinuation. Complete remission (CR) plus CR with partial hematologic recovery (CRh) rate was 42.4% (95% confidence interval [CI], 25.5% to 60.8%); CR 30.3% (95% CI, 15.6% to 48.7%). Median durations of CR+CRh and CR were not reached, with 95% CI lower bounds of 4.6 and 4.2 months, respectively; 61.5% and 77.8% of patients remained in remission at 1 year. With median follow-up of 23.5 months (range, 0.6-40.9 months), median overall survival was 12.6 months (95% CI, 4.5-25.7). Of 21 transfusion-dependent patients (63.6%) at baseline, 9 (42.9%) became transfusion independent. IDH1 mutation clearance was seen in 9/14 patients achieving CR+CRh (5/10 CR; 4/4 CRh). Ivosidenib monotherapy was well-tolerated and induced durable remissions and transfusion independence in patients with newly diagnosed AML. This trial was registered at www.clinicaltrials.gov as #NCT02074839.
Introduction
Historically, the standard-of-care treatment strategy for acute myeloid leukemia (AML) has included a choice between intensive or less-intensive induction, followed either by postremission hematopoietic stem cell transplantation or consolidation chemotherapy. Treatments are selected based on the patient’s performance status, medical comorbidities, and age, as well as biological features of the leukemia that predict response to treatment. Intensive induction generally includes an anthracycline-and-cytarabine−based regimen (so-called “7+3”), whereas lower-intensity regimens use low-dose cytarabine, decitabine, or azacitidine.1 Over the past several years, there have been incremental improvements to these baseline regimens. For example, selected AML patient populations benefit from the addition of gemtuzumab ozogamicin (CD33-calicheamicin conjugate)2 or midostaurin (FLT3 inhibitor)3 to standard “7+3” chemotherapy, whereas older or more frail patients benefit from the addition of venetoclax (B-cell lymphoma 2 [BCL-2] inhibitor)4 or glasdegib (hedgehog pathway inhibitor)5 to low-intensity chemotherapy. Despite these improvements, most patients with AML are still not cured, and survival is especially poor for patients unable to tolerate multiagent therapy.
Isocitrate dehydrogenase 1 (IDH1) is a metabolic enzyme that catalyzes the oxidative decarboxylation of isocitrate to α-ketoglutarate (α-KG). Mutations in IDH1 occur in ∼6% to 10% of patients with AML.6-8 Mutant IDH1 (mIDH1) catalyzes the neomorphic reduction of α-KG to the oncometabolite D-2-hydroxyglutarate (2-HG).9 2-HG competitively inhibits α-KG–dependent enzymes, leading to epigenetic alterations and impaired hematopoietic differentiation,10-12 and may also exert leukemogenic effects by inducing dependence on BCL-2.13 IDH1 mutations have been associated with adverse prognosis in patients with AML.14-16 Ivosidenib (formerly AG-120) is an oral, targeted, small-molecule inhibitor of mIDH1. The primary efficacy and safety data for patients with relapsed or refractory (R/R) AML receiving 500 mg of ivosidenib once daily in a phase 1 study have been published previously; in 125 patients, the rate of complete remission (CR) plus CR with partial hematologic recovery (CRh) was 30.4% and the median duration of CR+CRh was 8.2 months.17 Here, we report the outcomes for patients with newly diagnosed AML with an IDH1 mutation, ineligible for standard therapy, treated with 500 mg of ivosidenib daily, who were a subset of the patients enrolled in the phase 1 study. Based on the findings from this phase 1 study in patients with both R/R and newly diagnosed AML, ivosidenib is indicated for the treatment of AML with a susceptible IDH1 mutation, as detected by a US Food and Drug Administration−approved test, in adults with newly diagnosed AML who are ≥75 years old or who have comorbidities that preclude use of intensive induction chemotherapy, and in adults with R/R AML.18
Patients and methods
Study design
The design of this phase 1, multicenter, open-label, dose-escalation, and dose-expansion study has been reported previously.17 In brief, ivosidenib was administered orally, daily, in continuous 28-day cycles. In the dose-escalation phase, ivosidenib was administered at doses of 100 mg twice daily and 300, 500, 800, and 1200 mg once daily to establish the recommended phase 2 dose; 500 mg once daily was selected for the dose-expansion phase.
The study was conducted in accordance with the principles of the Declaration of Helsinki and good clinical practice guidelines, and the protocol was approved by the institutional review board/independent ethics committee at participating sites. Written informed consent was provided by all patients before screening and enrollment.
The study sponsor analyzed the data and conducted the statistical analyses. All authors had access to the primary clinical trial data on request.
Patients
Patients aged ≥18 years with an Eastern Cooperative Oncology Group performance-status (ECOG PS) of 0 to 2 and documented IDH1-mutated advanced hematologic cancer were eligible for inclusion. The dose-expansion phase comprised 4 arms that differed in eligibility criteria; patients with newly diagnosed IDH1-mutant AML who were ineligible for standard therapy were eligible for arm 2.
IDH1 mutation status was based on local laboratory testing with retrospective central laboratory confirmation in the dose-escalation phase; prospective central laboratory testing was required in the dose-expansion phase.
Safety and efficacy assessments
Treatment-emergent adverse events (AEs) were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE), version 4.03. Serious adverse events (SAEs) included those that resulted in death, were life threatening, led to hospitalization or prolongation of hospitalization, caused persistent or significant incapacity, or were deemed to be an important medical event.
Because ivosidenib is known to cause prolongation of the QT interval on electrocardiogram (ECG), concomitant use of cytochrome P-450 3A4 inhibitors and medications known to prolong the QT interval were permitted with approval by the medical monitor if careful monitoring of the QT interval was undertaken. Management guidelines included electrolyte repletion and adjustment of ivosidenib and/or relevant concomitant medications. ECG monitoring was conducted weekly, or more frequently based on institutional standards or investigator discretion, for the first 3 weeks following initiation of ivosidenib treatment of patients already taking moderate/strong CYP inhibitors, or following initiation of these agents.
Treatment with targeted mIDH inhibitors is associated with induction of differentiation of malignant cells and can lead to a clinical syndrome known as IDH differentiation syndrome (DS).19 DS was graded by investigators according to general NCI-CTCAE criteria with grades 1, 2, and 3 corresponding with mild, moderate, and severe. Guidelines for the management of DS were provided to investigators and details are included in the supplemental Appendix (available on the Blood Web site). Leukocytosis was reported by investigators according to general NCI-CTCAE criteria, and was observed in patients with and without co-occurring DS.
Clinical efficacy was assessed by the investigators using the 2003 modified International Working Group (IWG) response criteria for AML.20 In addition, CRh was defined per protocol as bone marrow myeloblasts of <5% combined with both absolute neutrophil count >500/μL and platelet count >50 × 109/L, and was derived by the sponsor. Other measures of clinical activity included duration of response, time to first response, and overall survival.
Translational analyses
Peripheral blood and bone marrow samples were collected at baseline for co-occurring mutation analysis. Samples collected in the dose-escalation phase were retrospectively analyzed by next-generation sequencing (NGS) using the FoundationOne Heme Panel (Foundation Medicine, Inc), which includes multiple probes to detect sites of the most frequently occurring mutations in a select panel of 405 genes.21 Samples collected in the dose-expansion phase were analyzed for comutations at Brigham and Women’s Hospital using the NGS 95-gene rapid heme panel.22
Longitudinal mIDH1 variant allele frequency (VAF) assessment for mutation clearance was performed. Bone marrow aspirates were collected at baseline and at specified time points during the study, processed to bone marrow mononuclear cells (BMMCs) via centrifugation, and viably frozen. For VAF assessment, the BEAMing digital polymerase chain reaction assay23 (OncoBEAM; Sysmex Inostics Inc) was used for evaluation of IDH1 mutations at position R132 (C/G/L/S/H). This method has a lower limit of detection for mIDH1 alleles of 0.02% to 0.04% (2 × 10−4 to 4 × 10−4) and is 50- to 100-fold more sensitive than NGS, making it a suitable assay for molecular minimal residual disease monitoring. Clearance of mIDH1 was defined as a reduction in mIDH1 VAF to below the limit of detection in BMMCs at ≥1 time point during the study in patients with detectable mIDH1 at baseline.
2-HG assessment was performed as reported in the supplemental Appendix.
Statistical analysis
The population of interest included all patients with newly diagnosed AML receiving 500 mg once daily of ivosidenib, in either the dose-escalation phase or arm 2 of the dose-expansion phase, and who received ≥1 dose of study treatment. One patient who was not confirmed by central laboratory to have an IDH1-R132 mutation by the companion diagnostic test (Abbott RealTime IDH1) was excluded from efficacy and translational analyses.
Time-to-event end points were estimated using Kaplan-Meier methods. Descriptive statistics were used for other clinical and laboratory variables.
Results
Patient characteristics
Overall, 258 patients with advanced hematologic malignancies (78 in the dose-escalation phase and 180 in dose-expansion) received ≥1 dose of ivosidenib in the study from 12 March 2014 to 8 May 2017. The cohort reported here comprises 34 patients with newly diagnosed AML who received ivosidenib 500 mg once daily (9 were treated in the dose-escalation phase and 25 in the dose-expansion phase). Thirty-three patients were positive for the IDH1-R132 mutation by the companion diagnostic test. As of the data cutoff date of 2 November 2018, 7 patients (21%) were still on treatment and 27 (79%) had discontinued owing to disease progression (n = 13; 38%), adverse event (n = 5; 15%), allogeneic stem cell transplant (n = 3; 9%), withdrawal of consent (n = 4; 12%), death (n = 1; 3%), and investigator decision (n = 1; 3%). Two patients (6%) remained in posttransplant follow-up. Full disposition details are included in supplemental Table 1. Baseline characteristics are provided in Table 1 and the supplemental Appendix.
Baseline characteristics of patients with newly diagnosed AML
| Characteristic | Ivosidenib 500 mg, N = 34 |
|---|---|
| Age, median (range), y | 76.5 (64-87) |
| Age category, n (%), y | |
| 60 to <75 | 15 (44) |
| ≥75 | 19 (56) |
| Women/men, n | 15/19 |
| ECOG PS at baseline, n (%) | |
| 0 | 8 (24) |
| 1 | 20 (59) |
| 2 | 5 (15) |
| 3 | 1 (3) |
| Nature of AML, n (%) | |
| De novo | 8 (24) |
| Secondary | |
| History of MDS | 18 (53) |
| History of MPD | 4 (12) |
| Treatment-related | 3 (9) |
| Other | 1 (3) |
| Prior hypomethylating agent, n (%) | 16 (47) |
| Cytogenetic risk status by investigator, n (%) | |
| Intermediate | 24 (71) |
| Poor | 9 (26) |
| Unknown | 1 (3) |
| Bone marrow blasts, median (range), % | 63 (1-97) |
| Hematology, n (%) | |
| White blood cells, ×109/L | |
| <15 | 28 (82) |
| 15 to <30 | 4 (12) |
| ≥30 | 2 (6) |
| Hemoglobin, g/L | |
| <80 | 5 (15) |
| ≥80 | 29 (85) |
| Platelets, ×109/L | |
| <50 | 21 (62) |
| ≥50 | 13 (38) |
| Transfusion dependent, n (%) | |
| Red blood cells | 16 (47) |
| Platelets | 14 (41) |
| Characteristic | Ivosidenib 500 mg, N = 34 |
|---|---|
| Age, median (range), y | 76.5 (64-87) |
| Age category, n (%), y | |
| 60 to <75 | 15 (44) |
| ≥75 | 19 (56) |
| Women/men, n | 15/19 |
| ECOG PS at baseline, n (%) | |
| 0 | 8 (24) |
| 1 | 20 (59) |
| 2 | 5 (15) |
| 3 | 1 (3) |
| Nature of AML, n (%) | |
| De novo | 8 (24) |
| Secondary | |
| History of MDS | 18 (53) |
| History of MPD | 4 (12) |
| Treatment-related | 3 (9) |
| Other | 1 (3) |
| Prior hypomethylating agent, n (%) | 16 (47) |
| Cytogenetic risk status by investigator, n (%) | |
| Intermediate | 24 (71) |
| Poor | 9 (26) |
| Unknown | 1 (3) |
| Bone marrow blasts, median (range), % | 63 (1-97) |
| Hematology, n (%) | |
| White blood cells, ×109/L | |
| <15 | 28 (82) |
| 15 to <30 | 4 (12) |
| ≥30 | 2 (6) |
| Hemoglobin, g/L | |
| <80 | 5 (15) |
| ≥80 | 29 (85) |
| Platelets, ×109/L | |
| <50 | 21 (62) |
| ≥50 | 13 (38) |
| Transfusion dependent, n (%) | |
| Red blood cells | 16 (47) |
| Platelets | 14 (41) |
MDS, myelodysplastic syndrome; MPD, myeloproliferative disease.
Safety
All 34 patients with newly diagnosed AML receiving 500 mg of ivosidenib once daily experienced treatment-emergent AEs, and 27 (79%) experienced a grade ≥3 AE (Table 2). The most commonly reported AEs (≥20% patients) of any grade, irrespective of relationship to ivosidenib, were diarrhea (n = 18; 53%), fatigue (n = 16; 47%), nausea (n = 13; 38%), decreased appetite (n = 12; 35%), leukocytosis (n = 9; 26%), anemia (n = 9; 26%), peripheral edema (n = 9; 26%), thrombocytopenia (n = 9; 26%), dizziness (n = 8; 24%), dyspnea (n = 8; 24%), hypomagnesemia (n = 8; 24%), arthralgia (n = 7; 21%), constipation (n = 7; 21%), epistaxis (n = 7; 21%), hypokalemia (n = 7; 21%), abdominal pain (n = 7; 21%), and insomnia (n = 7; 21%). Posterior reversible encephalopathy syndrome was reported in 1 patient (3%). The most commonly reported treatment-related AEs (≥10% patients) are reported in supplemental Table 2. The most commonly reported treatment-related grade ≥3 AEs were DS (n = 3; 9%), and ECG QT-prolonged, febrile neutropenia, and diarrhea (n = 2; 6% each). The most commonly reported SAEs (≥5% patients) were DS (n = 5; 15%), febrile neutropenia (n = 3; 9%), pneumonia (n = 3; 9%) ECG QT-prolonged (n = 2; 6%), and fatigue (n = 2; 6%). All SAEs of DS and ECG QT-prolonged, and febrile neutropenia in 1 patient (3%), were reported by investigators as treatment related.
Treatment-emergent AEs of any grade, irrespective of causality, reported in ≥20% of patients
| Patients with AE, n (%) | Ivosidenib 500 mg, N = 34 | |
|---|---|---|
| Any grade | Grade ≥3 | |
| Any AE | 34 (100) | 27 (79) |
| Diarrhea | 18 (53) | 2 (6) |
| Fatigue | 16 (47) | 4 (12) |
| Nausea | 13 (38) | 2 (6) |
| Decreased appetite | 12 (35) | 1 (3) |
| Thrombocytopenia | 9 (26) | 5 (15) |
| Anemia | 9 (26) | 4 (12) |
| Leukocytosis | 9 (26) | 1 (3) |
| Peripheral edema | 9 (26) | 0 |
| Dyspnea | 8 (24) | 1 (3) |
| Dizziness | 8 (24) | 0 |
| Hypomagnesemia | 8 (24) | 0 |
| Abdominal pain | 7 (21) | 1 (3) |
| Arthralgia | 7 (21) | 1 (3) |
| Constipation | 7 (21) | 1 (3) |
| Epistaxis | 7 (21) | 0 |
| Hypokalemia | 7 (21) | 1 (3) |
| Insomnia | 7 (21) | 0 |
| Patients with AE, n (%) | Ivosidenib 500 mg, N = 34 | |
|---|---|---|
| Any grade | Grade ≥3 | |
| Any AE | 34 (100) | 27 (79) |
| Diarrhea | 18 (53) | 2 (6) |
| Fatigue | 16 (47) | 4 (12) |
| Nausea | 13 (38) | 2 (6) |
| Decreased appetite | 12 (35) | 1 (3) |
| Thrombocytopenia | 9 (26) | 5 (15) |
| Anemia | 9 (26) | 4 (12) |
| Leukocytosis | 9 (26) | 1 (3) |
| Peripheral edema | 9 (26) | 0 |
| Dyspnea | 8 (24) | 1 (3) |
| Dizziness | 8 (24) | 0 |
| Hypomagnesemia | 8 (24) | 0 |
| Abdominal pain | 7 (21) | 1 (3) |
| Arthralgia | 7 (21) | 1 (3) |
| Constipation | 7 (21) | 1 (3) |
| Epistaxis | 7 (21) | 0 |
| Hypokalemia | 7 (21) | 1 (3) |
| Insomnia | 7 (21) | 0 |
AEs of special interest were defined as DS, leukocytosis, and ECG QT-prolonged. Among the 34 patients, DS was reported in 6 (18%), was grade ≥3 in 3 (9%), and led to dose interruptions in 3 patients (9%). The median time to onset of investigator-reported DS was 14.5 days (range, 8-82 days). Of the 6 patients with DS, 2 (33%) had co-occurring leukocytosis. Five patients (15%) had SAEs of DS, which were all considered to be treatment related. None of the DS events led to dose reductions, and no patients permanently discontinued ivosidenib due to DS. Treatment of DS included corticosteroids and diuretics, and hydroxyurea if accompanied by leukocytosis. Further details of the management guidelines are included in the supplemental Appendix. Best responses in the patients who experienced DS were 3 CR, 2 CRh, and 1 not assessed.
Leukocytosis of any grade occurred in 9 patients (27%) and was considered treatment related in 2 patients (6%). Grade ≥3 leukocytosis was reported in only 1 patient (3%) but was not considered treatment related in this patient.
ECG QT-prolonged was reported in 6 patients (18%), with 3 (9%) grade ≥3 events that were considered treatment related in 2 patients (6%). Dose interruptions and dose reductions for ECG QT-prolonged were reported in 4 patients (12%) and 2 patients (6%), respectively. No patients permanently discontinued ivosidenib due to ECG QT-prolonged. Treatment-related ECG QT-prolonged was reported as an SAE in 2 patients (6%).
Efficacy
Response
The median duration of treatment was 4.5 months (range, 0.3-40.9 months). The CR+CRh rate was 42.4% (14 of 33 patients; 95% confidence interval [CI], 25.5-60.8), the CR rate was 30.3% (10 of 33 patients; 95% CI, 15.6-48.7), and the overall response rate (ORR) was 54.5% (18 of 33 patients; 95% CI, 36.4-71.9; Table 3). The median durations of CR+CRh, CR, and overall response were not estimable (NE); the lower bounds of the 95% CIs were 4.6, 4.2, and 4.6 months, respectively. The estimated proportions of patients remaining in remission/response at 12 months were 61.5%, 77.8%, and 63.0% for CR+CRh, CR, and overall response, respectively. The median duration of CRh was 6.5 months (95% CI, 2.8 to NE).
Response rates in patients with newly diagnosed AML
| Response category | Ivosidenib 500 mg, n = 33* |
|---|---|
| CR + CRh rate, n (%) [95% CI] | 14 (42.4) [25.5-60.8] |
| Time to CR/CRh, median (range), mo | 2.8 (1.9-12.9) |
| Duration of CR/CRh, median [95% CI], mo | NE [4.6 to NE] |
| CR rate, n (%) [95% CI] | 10 (30.3) [15.6-48.7] |
| Time to CR, median (range), mo | 2.8 (1.9-4.6) |
| Duration of CR, median [95% CI], mo | NE [4.2 to NE] |
| CRh rate, n (%) [95% CI] | 4 (12.1) [3.4-28.2] |
| Time to CRh, median (range), mo | 3.7 (1.9-12.9) |
| Duration of CRh, median [95% CI], mo | 6.5 [2.8 to NE] |
| ORR by IWG, n (%) [95% CI]† | 18 (54.5) [36.4-71.9] |
| Time to first response, median (range), mo | 1.9 (0.9-3.6) |
| Duration of response, median [95% CI], mo | NE [4.6 to NE] |
| Best response by IWG, n (%) | |
| CR | 10 (30.3) |
| CRi or CRp | 6 (18.2) |
| PR | 1 (3.0) |
| MLFS | 1 (3.0) |
| SD | 10 (30.3) |
| PD | 3 (9.1) |
| Not assessed | 2 (6.1) |
| Response category | Ivosidenib 500 mg, n = 33* |
|---|---|
| CR + CRh rate, n (%) [95% CI] | 14 (42.4) [25.5-60.8] |
| Time to CR/CRh, median (range), mo | 2.8 (1.9-12.9) |
| Duration of CR/CRh, median [95% CI], mo | NE [4.6 to NE] |
| CR rate, n (%) [95% CI] | 10 (30.3) [15.6-48.7] |
| Time to CR, median (range), mo | 2.8 (1.9-4.6) |
| Duration of CR, median [95% CI], mo | NE [4.2 to NE] |
| CRh rate, n (%) [95% CI] | 4 (12.1) [3.4-28.2] |
| Time to CRh, median (range), mo | 3.7 (1.9-12.9) |
| Duration of CRh, median [95% CI], mo | 6.5 [2.8 to NE] |
| ORR by IWG, n (%) [95% CI]† | 18 (54.5) [36.4-71.9] |
| Time to first response, median (range), mo | 1.9 (0.9-3.6) |
| Duration of response, median [95% CI], mo | NE [4.6 to NE] |
| Best response by IWG, n (%) | |
| CR | 10 (30.3) |
| CRi or CRp | 6 (18.2) |
| PR | 1 (3.0) |
| MLFS | 1 (3.0) |
| SD | 10 (30.3) |
| PD | 3 (9.1) |
| Not assessed | 2 (6.1) |
CRi, CR with incomplete hematologic recovery; CRp, CR with incomplete platelet recovery; MLFS, morphologic leukemia-free state; NE, not estimable; ORR, overall response rate; PD, progressive disease; PR, partial response; SD, stable disease.
One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses.
ORR = CR + CRi + CRp + PR + MLFS. IWG responses, including CR, were reported by investigators. CRh was derived by the sponsor and defined as bone marrow myeloblasts of <5% combined with both absolute neutrophil count >500/μL and platelet count >50 × 109/L.
For 7 patients achieving CR or CRh who remained on ivosidenib treatment at data cutoff, response duration ranged from 15.7 to 35.9 months.
The median time (range) to response was 2.8 months (1.9-12.9 months) for CR+CRh, 2.8 months (1.9-4.6 months) for CR, 3.7 months (1.9-12.9 months) for CRh, and 1.9 months (0.9-3.6 months) for overall response. Individual best overall responses and duration of treatment of the 33 patients included in the efficacy analysis are shown in Figure 1A.
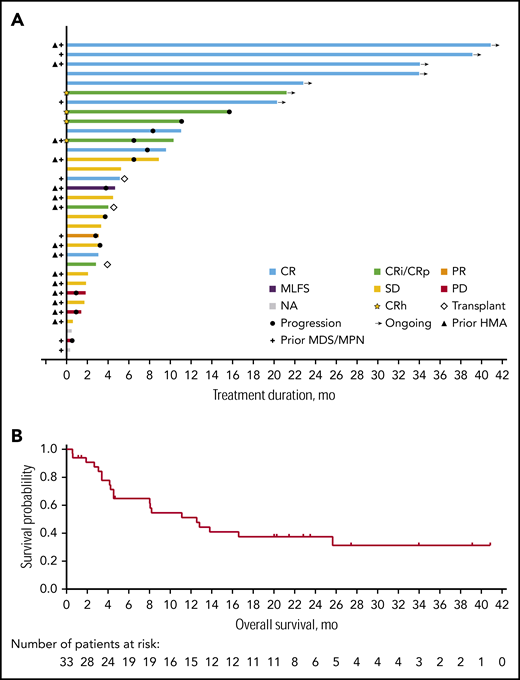
Treatment responses and overall survival. (A) Duration of treatment and best overall response (n = 33*). (B) Kaplan-Meier estimate for overall survival (n = 33*). *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses. CRi, CR with incomplete hematologic recovery; CRp, CR with incomplete platelet recovery; HMA, hypomethylating agent; MDS, myelodysplastic syndrome; MLFS, morphologic leukemia-free state; MPN, myeloproliferative neoplasm; NA, not assessed; PD, progressive disease; PR, partial response; SD, stable disease.
Treatment responses and overall survival. (A) Duration of treatment and best overall response (n = 33*). (B) Kaplan-Meier estimate for overall survival (n = 33*). *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses. CRi, CR with incomplete hematologic recovery; CRp, CR with incomplete platelet recovery; HMA, hypomethylating agent; MDS, myelodysplastic syndrome; MLFS, morphologic leukemia-free state; MPN, myeloproliferative neoplasm; NA, not assessed; PD, progressive disease; PR, partial response; SD, stable disease.
In the 15 patients who had received a prior hypomethylating agent (HMA) for an antecedent hematologic disorder, the rate of CR+CRh was 26.7% (4 of 15 patients; 95% CI, 7.8-55.1), and CR was 20.0% (3 of 15 patients; 95% CI, 4.3-48.1). The median duration of CR+CRh was not achieved (NE [95% CI, 4.6, NE]). In the 18 patients without prior HMA treatment, the CR+CRh rate was 55.6% (10 of 18 patients; 95% CI, 30.8-78.5), and CR 38.9% (7 of 18 patients; 95% CI, 17.3-64.3). The median duration of CR+CRh was not achieved (NE [95% CI, 2.8-NE]).
The CR+CRh rate was consistent across other subgroups evaluated including age, sex, region, race, baseline ECOG PS, prior history of myelodysplastic syndrome, baseline cytogenetics and cytogenetic risk status, and IDH1 mutation type. However, interpretation of these subgroup results should be made with caution owing to the small sample size.
Overall survival
With a median follow-up of 23.5 months (range, 0.6-40.9 months), median overall survival was 12.6 months (95% CI, 4.5-25.7). The estimated 12-month overall survival rate was 51.1% (Figure 1B).
Hematologic analysis
In this population of patients with newly diagnosed AML treated with ivosidenib, the mean hematologic parameters improved over time. The mean absolute neutrophil count, hemoglobin, and platelet values increased coincident with a reduction in bone marrow aspirate blasts (Figure 2). Acquisition and maintenance of transfusion independence were observed across response categories. Of the 33 newly diagnosed patients, 21 (63.6%) were dependent on red blood cell and/or platelet transfusions at baseline. Of these, 9 (42.9%) became transfusion independent for a period of ≥56 days during treatment (Figure 3). Among the 12 patients (36.4%) who were transfusion independent at baseline, transfusion independence was maintained for a period of ≥56 days during treatment in 7 patients (58.3%).
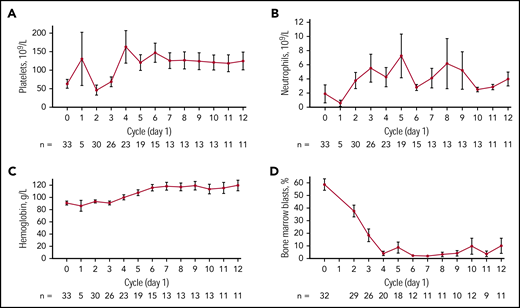
Mean ± standard deviation hematologic parameters over time (n = 33*). (A) platelet count, (B) absolute neutrophil count, (C) hemoglobin level, and (D) percentage of bone marrow blasts over time. *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses.
Mean ± standard deviation hematologic parameters over time (n = 33*). (A) platelet count, (B) absolute neutrophil count, (C) hemoglobin level, and (D) percentage of bone marrow blasts over time. *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses.
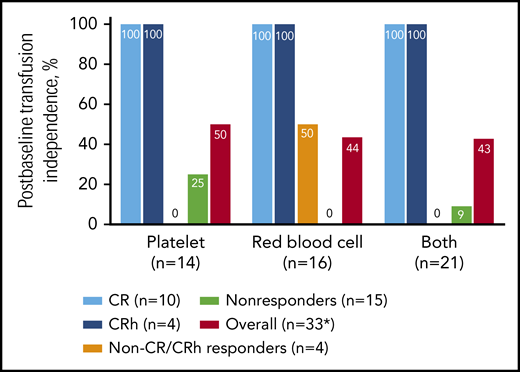
Transfusion independence in patients who were transfusion dependent at baseline. Non-CR/CRh responders include patients with CR with incomplete hematologic recovery/incomplete platelet recovery and morphologic leukemia-free state not meeting the criteria for CRh, and patients with PR. Nonresponders include patients with stable disease and progressive disease. *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses.
Transfusion independence in patients who were transfusion dependent at baseline. Non-CR/CRh responders include patients with CR with incomplete hematologic recovery/incomplete platelet recovery and morphologic leukemia-free state not meeting the criteria for CRh, and patients with PR. Nonresponders include patients with stable disease and progressive disease. *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses.
Translational findings
The most frequent co-occurring mutations at baseline were ASXL1, DNMT3A, RUNX1, SRSF2, TET2, and NRAS (supplemental Figure 1). In this limited data set, no single gene mutation was significantly associated with clinical response to ivosidenib treatment. Receptor tyrosine kinase (RTK) pathway mutations (NRAS, FLT3, PTPN11, KRAS) were not observed in any of the 14 patients achieving CR/CRh responses, compared with 7 of 19 patients (36.8%) with a non-CR/CRh response or no response (P = .01; Figure 4). Comutation burden and relationship to response is reported in the supplemental Appendix.
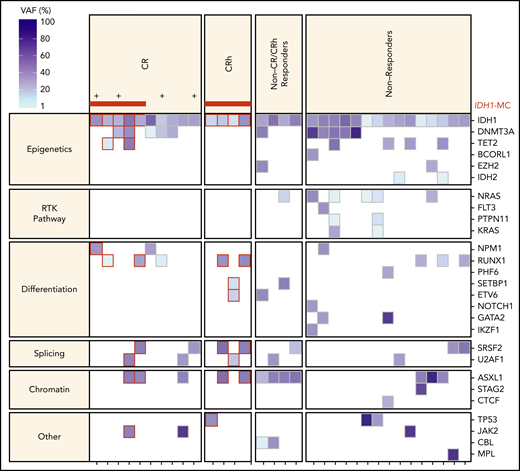
Baseline co-occurring mutations by functional category and clinical response status (n = 33*). RTK pathway mutations were not observed in patients achieving CR/CRh responses (P = .01 by Fisher exact test). *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses. + indicates patients with treatment duration of >32 months. Red horizontal bars indicate IDH1 mutation clearance. IDH-MC, IDH-mutation clearance.
Baseline co-occurring mutations by functional category and clinical response status (n = 33*). RTK pathway mutations were not observed in patients achieving CR/CRh responses (P = .01 by Fisher exact test). *One patient enrolled in dose-escalation phase was positive for the IDH1-D54N mutation by local testing and was not positive for the IDH1-R132 mutation by the companion diagnostic test; this patient was therefore excluded from the efficacy analyses. + indicates patients with treatment duration of >32 months. Red horizontal bars indicate IDH1 mutation clearance. IDH-MC, IDH-mutation clearance.
Baseline mIDH1 allele frequency was not significantly associated with the achievement of a CR or CRh response. Mean baseline allele frequency was 33.3% (range, 13.2% to 58.3%) in patients achieving CR/CRh (n = 14) and 34.1% (range, 3.6% to 57.6%) in patients with all other responses including nonresponders (n = 19; P = .689). Longitudinal IDH1 mutation status was evaluated in 30 patients. IDH1 mutation clearance in BMMCs was observed in 9 of 14 patients (64.3%) with a best response of CR+CRh (5 of 10 patients with CR and 4 of 4 with CRh; supplemental Table 3). In contrast, IDH1 mutation clearance in BMMCs was not observed in any patients with newly diagnosed AML who did not achieve CR or CRh (n = 16). IDH1 mutation clearance was significantly associated with CR+CRh (P < .001; Fisher exact test for CR+CRh vs other responses [non-CR/CRh responses and no response]).
Analysis of mean 2-HG levels at each time point showed a substantial reduction by day 8 of cycle 1 that was maintained throughout treatment in patients with newly diagnosed AML (supplemental Figure 2).
Discussion
Patients with newly diagnosed AML and an IDH1 mutation who are ineligible for standard therapy based on advanced age and/or comorbidities represent a molecularly defined population with poor prognosis and limited treatment options. In this study, 56% of patients were aged ≥75 years, 47% had prior exposure to HMAs, and 76% had secondary AML. Although the authors acknowledge the open-label, nonrandomized design, and small sample size of this study, 500 mg of ivosidenib once daily was well tolerated among these older patients with high-risk AML, and the majority of observed AEs were expected for this population. The safety profile was also favorable relative to currently available therapies for AML, including low-dose cytarabine and HMAs when used alone, and in particular, when combined with newly available agents.5,24 Ivosidenib-specific AEs of DS, ECG QT-prolonged, and leukocytosis were managed with appropriate guidance, and no patients with newly diagnosed AML permanently discontinued treatment due to these AEs. DS was managed by dose interruption and treatment with corticosteroids, diuretics, and oral hydroxyurea as needed. Health care professionals should be aware that this AE can result from ivosidenib use, but that it can be managed with hemodynamic monitoring and standard treatment as outlined in the ivosidenib US package insert.18 The frequencies of ivosidenib-specific AEs observed in this newly diagnosed AML population were similar to those seen in the R/R AML population, as were the frequencies of the most common treatment-related grade ≥3 AEs.
Single-agent ivosidenib, 500 mg once daily, induced durable responses, with a CR+CRh rate of 42.4% (median duration in months, NE; 95% CI, 4.6 to NE) and a CR rate of 30.3% (median duration in months, NE; 95% CI, 4.2 to NE). As expected, the CR+CRh and CR rates appear higher in the mIDH1 newly diagnosed population compared with the mIDH1 R/R AML population in this study,17 though as noted herein, the newly diagnosed AML subgroup in this study is small. Among other recently available therapies for patients with newly diagnosed AML, preliminary favorable responses have been seen in the small subset of patients with IDH mutations treated with the combination of venetoclax plus HMAs, and further data on the efficacy of this combination in mIDH1 subgroups are anticipated.24 Additionally, in the present study, responses were observed in patients who had received a prior HMA, with a CR+CRh rate of 26.7%, indicating that ivosidenib monotherapy is a treatment option for these patients who were ineligible for standard therapy for AML. Transfusion independence, which clinicians and patients associate with improved quality of life, was achieved across all response categories (including those without a response). Furthermore, 7 of the 12 patients who were transfusion independent at diagnosis remained transfusion independent despite treatment, which does not generally occur with other available treatments.
Ivosidenib induced IDH1 mutation clearance in 5 of 10 patients with CR and all 4 patients with CRh. The association between IDH1 mutation clearance and CR/CRh responses suggests that treatment with ivosidenib monotherapy alters the biology of newly diagnosed mIDH1 AML. In this subgroup, all but 1 patient with an RTK pathway mutation were nonresponders. Similarly, we previously reported that RTK pathway mutations are associated with lack of response to ivosidenib in patients with mIDH1 R/R AML.17 Nonetheless, responses in patients with RTK mutations were observed in a small proportion of patients with mIDH1 R/R AML,17 and in 1 patient in the mIDH1 newly diagnosed subgroup reported here, suggesting that RTK pathway mutations do not preclude clinical response to ivosidenib. This raises the possibility that combining ivosidenib with pharmacologic agents capable of inhibiting the RTK pathway may improve clinical outcomes for patients.
Ivosidenib monotherapy resulted in promising response rates and significant clinical benefit in patients with newly diagnosed AML ineligible for standard therapy, including patients aged ≥75 years and those with comorbidities precluding intensive chemotherapy. It is important to note that the patient population reported here included a high proportion of patients with secondary AML and patients who had received prior treatment with an HMA for an antecedent hematologic disorder, both of which are patient populations with poor responses to cytotoxic therapies. Thus, ivosidenib is a compelling treatment option on the basis of responses in high-risk patients (including those with prior HMA treatment), once-daily oral dosing, and a favorable safety profile. Furthermore, more than one-half of responders achieved IDH1 mutation clearance. Finally, as ivosidenib is not associated with myelotoxicity, responding patients could receive prolonged treatment without incurring the severe cytopenias characteristic of multiagent chemotherapy for AML. The ease of administration, favorable toxicity profile, and lack of myelosuppression make ivosidenib an excellent potential combination partner and several additional studies are planned or under way to further evaluate ivosidenib in a variety of combinations in patients with newly diagnosed AML, including with azacitidine (phase 3, NCT03173248 and phase 1, NCT02677922), with standard AML induction and consolidation therapy (phase 1, NCT02632708), and with venetoclax (phase 1, NCT03471260).
Investigators interested in data sharing and collaboration should contact the corresponding author.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
Medical writing assistance was provided to the authors by Helen Varley (Excel Medical Affairs, Horsham, United Kingdom).
This work was supported by funding, for research and medical writing assistance, from Agios Pharmaceuticals, Inc.
Authorship
Contribution: K.E.Y., S.V.A., B.W., and E.C.A. designed the study; S.M.K., H.L., S.V.A., B.W., and E.C.A. developed the protocol; H.L. developed the statistical analysis plan; G.J.R., C.D.D., E.M.S., S.d.B., A.S.M., G.T.P., J.K.A., M.L.A., W.D., H.P.E., G.N.M., D.A.P., A.S.S., G.L.U., J.M.W., A.T.F., H.M.K., M.S.T., and R.M.S. participated in recruitment of patients and collection of data; K.E.Y., S.M.K., D.H., H.L., S.V.A., and E.C.A. analyzed the clinical data; G.J.R., C.D.D., E.M.S., S.d.B., A.S.M., G.T.P., J.K.A., M.L.A., W.D., H.P.E., G.N.M., D.A.P., A.S.S., G.L.U., J.M.W., A.T.F., H.M.K., M.S.T., V.Z., K.E.Y., S.M.K., D.H., H.L., S.V.A., E.C.A., and R.M.S. participated in clinical data interpretation; S.C., D.D., B.F., H.W., V.Z., B.W., and E.C.A. participated in the analysis and interpretation of pharmacodynamic and translational data; and G.J.R., C.D.D, H.L., and E.C.A. oversaw drafting of the manuscript; and all authors participated in manuscript development and final approval of the submitted version.
Conflict-of-interest disclosure: G.J.R. is a consultant/advisor to or was on a data and safety monitoring committee for AbbVie, Actinium, Agios, Amphivena, Argenx, Astex, Astellas, Bayer, Celgene, Celltrion, Daiichi Sankyo, Eisai, Janssen, Jazz Pharmaceuticals (Jazz), Novartis, MEI Pharma, Orsenix, Otsuka, Pfizer, Roche/Genentech, Sandoz, Takeda, and Trovagene; and received research funding from Cellectis. C.D.D. is a consultant/advisor to Agios and Celgene; received honoraria from AbbVie, Agios, Bayer, Celgene, Karyopharm Therapeutics, and MedImmune; and received research funding from AbbVie, Agios, Celgene, and Daiichi Sankyo. E.M.S. is a stockholder in/has ownership of Auron Therapeutics; is a consultant/advisor to AbbVie, Agios, Astellas, Bayer, BioLineRx, Celgene, Daiichi Sankyo, Genentech, Novartis, Pfizer, PTC Therapeutics, and Syros; received research funding from Agios, Amgen, Bayer, Celgene, and Syros; and received travel expenses from AbbVie, Astellas Pharma, Celgene, Daiichi Sankyo, Novartis, and Syros. S.d.B. received honoraria from, is a consultant/advisor to, and received research funding and travel expenses from Agios; received honoraria from, and was on a speakers’ bureau for, AbbVie; received honoraria from, and was a consultant/advisor to, Bayer; and received honoraria from, was a consultant/advisor to, and received travel expenses from Carthagenetics, Celgene, FORMA Therapeutics, Novartis, Pfizer, Pierre Fabre, Seattle Genetics, and Servier. A.S.M. is a consultant/advisor to AbbVie, Agios, Astellas, Jazz, and PTC Therapeutics; and was on a speakers’ bureau for Novartis. J.K.A. is a consultant/advisor to AbbVie, Agios, Cancer Expert Now, Daiichi Sankyo, Glycomimetics, Novartis, and Theradex; was on speakers’ bureaus for PeerView, prIME Oncology, and the France Foundation; and received institutional research funding from Agios, Astellas, Boehringer Ingelheim, Celgene, FujiFilm, and Genentech. M.L.A. received research funding from Cephalon. H.P.E. is a consultant/advisor to, was on a speakers’ bureau for, and received research funding from Agios; is a consultant/advisor to, was on a speakers’ bureau for, and provided other services to Celgene; is a consultant/advisor to, provided other services for, and received research funding from GlycoMimetics; is a consultant/advisor to, and received research funding from, Amgen, Daiichi Sankyo, Immunogen, Pfizer, and Seattle Genetics; is a consultant/advisor to, and was on speakers’ bureaus for Incyte, Jazz, and Novartis; is a consultant/advisor to Astellas and Macrogenics; and received research funding from Janssen, Juno Therapeutics, and Takeda. G.N.M. is a consultant/advisor to AbbVie, Amgen, Curis, Forty Seven Inc, Jazz, and NKarta; and received research funding from Agios and Juno Therapeutics. D.A.P. is a consultant/advisor to, and received research funding from, Agios and Pfizer; and is a consultant/advisor to AbbVie, argenx, Celgene, Celyad, Curis, and Servier. A.S.S. was on speakers’ bureaus for Amgen and Celgene. G.L.U. is a consultant/advisor to Curis, Glycomimetics, Jazz, Novartis, Novo Nordisk, and Pfizer; and received travel expenses from Novartis. J.M.W. received research funding from Takeda; was on a speakers’ bureau for, and a consultant/advisor to, Jazz; and is a consultant/advisor to Celgene and Pfizer. A.T.F. is a consultant to Agios, Astellas, Daiichi Sankyo, Celgene, Takeda, Trovagene, Jazz, and Boston Biomedical; and received research funding from Agios, Celgene, Exelixis, and Takeda. H.M.K. received honoraria and research funding from Amgen, ARIAD, Bristol-Myers Squibb, and Pfizer; received honoraria from AbbVie, Immunogen, and Orsenix; and received research funding from Astex and Novartis. M.S.T. has patents with/received royalties from/holds intellectual property (IP) with UpToDate; was a consultant/advisor for, and received research funding from, AbbVie, Arog, Biosight, Cellerant, and Orsenix; received research funding from ADC Therapeutics; and is a consultant/advisor to Bioline Rx, Daiichi Sankyo, DeltaFly Pharma, KAHR Medical, NOHLA Therapeutics, and Rigel. S.C., B.F., H.W., V.Z., S.M.K., and H.L. are employed by and are stockholders in Agios. D.H. is a consultant/advisor to Agios, and was employed by, and a stockholder in, Agios at time of study. D.D., K.E.Y., and S.V.A. were employed by, and stockholders in, Agios at time of study. B.W. is employed by, is a stockholder in, and holds patents with Agios. E.C.A. was employed by, and a stockholder in, Agios at time of study; and provided consulting services to Advance Medical. R.M.S. received honoraria from DAVA, Medscape, Prime Oncology, and Research to Practice; was a consultant/advisor for, and received research funding from, AbbVie, Agios, and Novartis; and was a consultant/advisor to Actinium, Amgen, argenx, Arog, Astellas, AstraZeneca, BioLineRx, Celgene, Cornerstone, Genentech/Roche, Jazz, Macrogenics, Otsuka, Pfizer, Stemline Therapeutics, Takeda, and Trovagene. The remaining authors declare no competing financial interests.
The current affiliation for H.P.E. is Duke University, Durham, NC.
The current affiliation for G.N.M. is Stanford University, Stanford, CA.
David Dai died on 9 August 2019.
Correspondence: Gail J. Roboz, Weill Cornell Medical College, 520 East 70th St, Starr Pavilion, 3rd Fl, New York, NY 10021; e-mail: gar2001@med.cornell.edu.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal