


Background In myelodysplastic syndromes (MDS), chronic myelomonocytic leukemia (CMML) and acute myeloid leukemia (AML), achievement of morphologic complete response (CR) is a prerequisite for potential cure. In AML, CR is deemed the major outcome associated with improved overall survival (OS); patients (pts) without CR are considered non-responders, and hematologic improvement (HI) without bone marrow blast (BMB) clearance is considered treatment (trt) failure (Cheson 2003). Evidence suggests that these definitions may not be applicable to older pts treated with hypomethylating agents (HMA), and that achievement of CR may not be necessary for prolonged OS (Pleyer 2013, 2014, 2015; Schuh 2015; Bloomfield 2018).
IWG response criteria for HI do not differentiate between pts who qualify for response (QFR) vs those that do not. Pts with 'normal' blood counts at trt start are per definition HI non-responders. This may obscure potential survival benefits of responding pts.
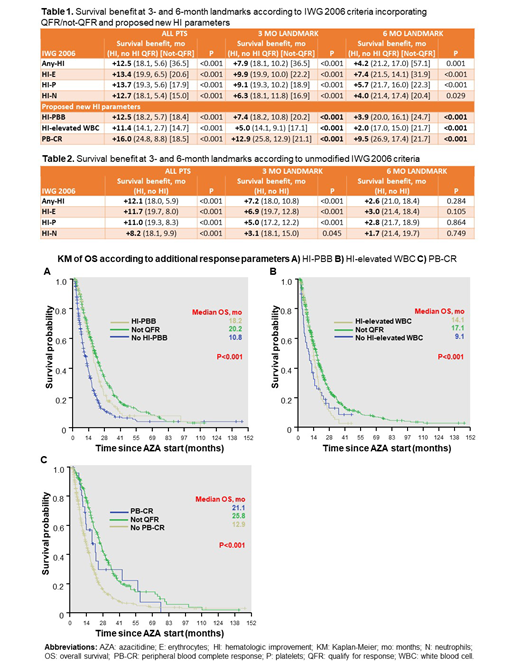
Aims 1) Assess the impact of HI irrespective of BMB clearance and excluding immortal time bias via landmark analyses. 2) Differentiate between pts who QFR, and those with 'normal' baseline values (not-QFR) defined according to IWG prerequisites for CR. 3) Introduce 3 new categories of HI: peripheral blood blasts (PBB), elevated white blood cells (WBC), and PB-CR (defined as Hb ≥11 g/dl, ANC ≥1.0 G/l, WBC <15 G/l, PB blasts: 0%) in analogy to the concept of complete hematologic response in chronic myelogenous leukemia.
Methods 1301 consecutive pts with azacitidine (AZA) trt were analyzed (NCT01595295). Data cut-off 26.07.19. HI was assessed according to IWG criteria (Cheson 2006) and the definitions specified in 3) above. More recent proposals of revision for low-risk MDS pts included in trials (Platzbecker 2018) remain largely idem. Human errors in HI assessment for each AZA cycle and lineage were excluded by automated computational calculation from electronic case report form (eCRF) data. Landmark analyses were performed at 3 months (mo) (HI requires ≥8 weeks response duration) and 6 mo (91, 92 and 88% of MDS, CMML and AML pts respond by cycle 6 [Silverman 2011; Pleyer 2013, 2014]). Statistics were performed by Unidata Geodesign GmbH using DeployR Open 8.0.0.
Results In total, 462, 113, and 720 pts had MDS, CMML and AML (n=6 unknown). At AZA start, median age was 73 (range 23-93) years. One, 2 or 3 cytopenias were present in 25, 41 and 29% of pts and 46% were transfusion dependent. 55% received AZA 1st line (26% of whom received prior growth factors or iron chelators). Median AZA dose was 889 mg/cycle and 73 mg/m2/day. Median time to 1st response was 3.0 mo and 95% of pts responded by cycle 6. During AZA trt 1091 BM evaluations (BME) were performed in 599 (46%) pts. At the 3 (6) mo landmark, 44% (47%) of pts with BME achieved CR or CR with incomplete blood count recovery (CRi). Early mortality was 5.6 and 10.3% at 30 and 60 days.
Of 932 (598) pts that met the 3 (6) mo landmark, a total of 39% (25%) had no BME. The impact of HI on OS became smaller the later the landmark (Tables 1 and 2). The impact of response on OS was 0.4-4.4 mo longer and significance at the 6 mo landmark was retained using IWG criteria with (Table 1) vs without (Table 2) differentiating between pts who did or did not QFR. Pts who did not QFR had similar or better OS compared with responders. At the 3 mo landmark, proposed additional response parameters HI-PBB, HI-elevated WBC and PB-CR were assoc. with a survival benefit of +7.4, +5.0 and +12.9 mo (Table 1, Fig 1A-C).
Conclusions
1) The impact of HI on OS is overestimated without landmark analyses. Median time to 1st response was 3.0 mo and ≥8 weeks response duration required. We therefore suggest using a 3 mo landmark when assessing HI. 2) Using IWG criteria for HI assessment underestimates the impact of response, as non-responders are diluted by pts who do not QFR. Distinguishing QFR/not-QFR seems necessary. 3) Proposed additional HI categories (HI-PBB, HI-elevated WBC, PB-CR) add value to current response criteria. It is often the case that BME are not performed in elderly pts in real-world settings (Dinmohamed 2015; current study). Achievement of HI in any lineage and especially PB-CR might be used as a surrogate for response in pts unable or unwilling to undergo BME for response assessment. This large and growing database is suitable to allow future validation of potential novel response criteria.
Pleyer:Celgene: Other: Advisory board; Novartis: Other: Advisory board; Inflection Point Biomedical Advisors: Other: Advisory board; Agios: Other: Advisory board; Abbvie: Other: Advisory board. Pfeilstocker:Novartis: Consultancy, Honoraria; Janssen-Cilag: Honoraria; Celgene: Consultancy, Honoraria. Stauder:Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Teva (Ratiopharm): Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Advisory board, Research Funding. Heibl:Daiichi Sankyo: Honoraria; Pfizer: Honoraria; Mundipharma: Honoraria; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; AOP Orphan Pharmaceuticals: Honoraria, Membership on an entity's Board of Directors or advisory committees; Roche: Honoraria; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees. Sill:Astex: Other: Advisory board; Novartis: Other: Advisory board; AbbVie: Other: Advisory board; Astellas: Other: Advisory board. Girschikofsky:Pfizer: Honoraria, Research Funding; Mundipharma: Consultancy, Honoraria. Petzer:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; Roche: Other: Personal fees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees. Vallet:MSD: Honoraria; Pfizer: Honoraria; Roche Pharmaceuticals: Consultancy. Geissler:Abbvie: Honoraria; Pfizer: Honoraria; Amgen: Honoraria; AstraZeneca: Honoraria; AOP: Honoraria; Celgene: Honoraria; Novartis: Honoraria; Roche: Honoraria; Ratiopharm: Honoraria. Sperr:Novartis: Honoraria; Celgene: Consultancy, Honoraria. Leisch:Novartis: Honoraria, Other: Travel support; Celgene: Other: Travel support; Bristol-Myers-Squibb: Honoraria. Egle:Celgene: Honoraria, Other: Advisory board and Travel support. Melchardt:MSD: Honoraria; Merck: Honoraria, Research Funding; Takeda: Honoraria; Janssen-Cilag: Honoraria; Roche: Honoraria; Novartis: Honoraria; Cephalon: Research Funding. Piringer:Amgen: Research Funding; Roche: Other: Travel support; Merck: Other: Travel support; Bayer: Research Funding. Zebisch:Roche: Honoraria; Novartis: Honoraria, Other: Advisory board; Celgene: Honoraria; AbbVie: Other: Advisory board. Machherndl-Spandl:Celgene: Other: Advisory board. Wolf:Celgene: Honoraria, Research Funding; Abbvie: Honoraria. Keil:Bionorica: Honoraria, Research Funding; Roche: Honoraria; Pfizer: Honoraria; Celgene: Honoraria; AbbVie: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Daiichi Sankyo: Honoraria; Novartis: Honoraria; Merck: Honoraria, Research Funding; Takeda: Honoraria, Research Funding. Greil:Ratiopharm: Research Funding; MSD: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; Novartis: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Cephalon: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; Gilead: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; Pfizer: Honoraria, Research Funding; Bristol-Myers-Squibb: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; Genentech: Honoraria, Research Funding; Merck: Consultancy, Honoraria, Research Funding; Eisai: Honoraria; Mundipharma: Honoraria, Research Funding; Sanofi Aventis: Honoraria; Takeda: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; GSK: Research Funding; Sandoz: Honoraria; Daiichi Sankyo: Consultancy, Honoraria; Janssen-Cilag: Honoraria; Amgen: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; Roche: Consultancy, Honoraria, Other: Travel/accomodation expenses, Research Funding; Boehringer Ingelheim: Honoraria.
Azacitidine is not approved for the treatment of MP-CMML, CMML with <10% BM blasts and IPSS low-risk MDS in the EU
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal