

Introduction:
The CARPALL study (NCT02443831) employed a novel CD19CAR (CAT-41BBz CAR) with a faster off rate than the Kymriah FMC63-41BBz CAR (CAT 3.1x10-3s-1, FMC 6.8 x 10-5s-1), with equivalent on-rate (CAT 2.2 x 105, FMC 2.1 x 105). We herein report updated outcomes and CAR T cell persistence with an additional 6 months follow up from a submitted manuscript (Ghorashian et al., Nat Med, submitted)
Methods:
Patients aged <25 years with high risk, relapsed CD19+ B-ALL were eligible on this multi-centre, open label, non-randomised phase I study of autologous CAT-41BBz CAR T cells. Patients were followed to a data cut-off of 07/18/2019.
CAT-41BBz CAR T cells were generated by magnetic bead activation of leucapheresed PBMCs, lentiviral transduction, followed by bioreactor expansion and magnetic bead removal prior to cryopreservation.
All patients received lymphodepletion (fludarabine + cyclophosphamide) followed by 1x106/kg CAR T cells. Presence of CAR T cells in the blood and bone marrow (BM) was assessed (flow cytometry and qPCR) monthly for 6 months, then 6 weekly to 1 year and then 3 monthly. BM MRD was assessed (IgH qPCR, flow cytometry) at the same time-points up to 2 years to establish durability of responses as a stand-alone therapy. Primary end-points were incidence of grade 3-5 toxicity and the proportion of patients achieving molecular remission.
Results:
Of 17 patients recruited, 14 were treated due to manufacturing failure in 3 patients.The median age was 9 years (range 1-19 years). All patients had advanced ALL with a median of 4 prior therapy lines. 10 of 14 patients (71%) had relapsed post allogeneic SCT. Prior to lymphodepletion, 4 patients had >5% BM disease, 6 had disease between 5x10-2and 1x10-5, 4 were BM MRD negative having had recurrent isolated CNS disease. Median transduction efficiency was 31% (range 16.5 to 96.4%). 12/14 treated patients received the anticipated dose of 1x106CAR T cells/kg (2 received 0.9x106/kg).
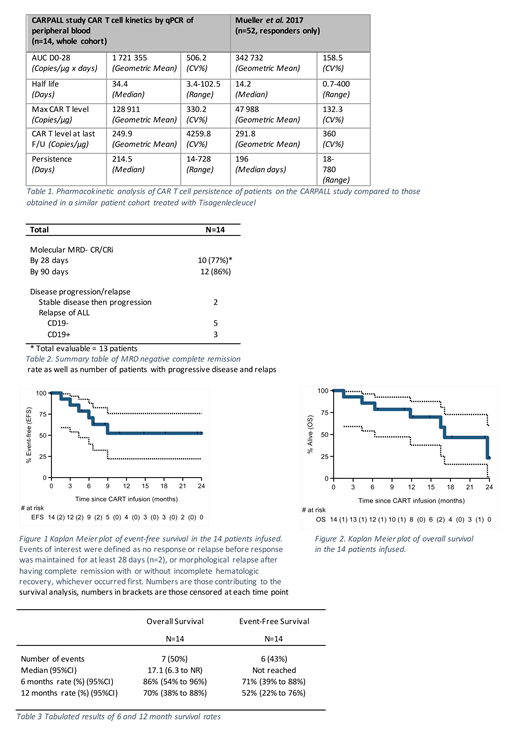
Considering all evaluable patients, (n=14 for CAR T cell persistence by qPCR, n=13 by flow) the geometric mean of Cmax was 128 912/µg DNA and of the area under the curve between D0 and D28 was 1,721,355 copies/ µg DNA (Table 1). At the point of maximal expansion, a median of 35% of circulating T cells were CAR+. Median half-life was 34 days (range 3-102). CAR T cells continued to be detectable by qPCR in 11 of 14 (79%) patients at last assessment and by flow cytometry up to 30 months post infusion in 8 of 13(61%). Median duration of CAR T persistence by flow was 261 days (range 7-917). 3 patients failed to have persistence of CAR T cells beyond 1 month. T cell mediated anti-CAR specific cytotoxic activity was detected in 2/2 evaluable patients. Updated persistence data will be presented at the meeting
Cytokine release syndrome (CRS) occurred in 13 (93%, grade 1 n=9, grade 2 n=4). None developed ≥grade 3 CRS, had CRS-related ICU admission, or received Tocilizumab. CRS was associated with modest elevations of IL-6, IFN-γand IL-10. Grade 2 neurotoxicity was observed in 3 patients and resolved spontaneously. One patient had grade 4 leucoencephalopathy presumed due to chemotherapy as well as grade 5 sepsis. Ten patients (71%) had grade 3-4 cytopenia persisting beyond day 28 or recurring afterthis.
12/14 (86%) patients achieved molecular complete or continuing complete remission at a median of 30 days post infusion (range 30-90 days, Table 2). At a median follow-up of 20.3 months, 4/14 (29%) evaluable patients remain MRD negative. 5 relapsed with CD19-disease, 1 with CD19+ disease. The median duration of EFS (based on death or morphological relapse) has not been reached, 12 month EFS = 52%, OS = 70% (Figures 1, 2 and Table 3).
Conclusion:
We noted excellent CAR T cell expansion and persistence in a ALL cohort treated with the fast off-rate CAT-41BBz CAR despite their lower BM disease at treatment compared to other studies. The kinetics documented for all evaluable patients showed a 5-fold greater CAR T cell expansion and 2-fold longer half-life than responders in published series utilising tisagenlecleucel in a similar ALL cohort (Mueller et al., Blood 2017). Patients had a favourable toxicity profile with no severe (grade 3-4) CRS and equivalent disease outcomes to the ELIANA study despite having similarly advanced disease (Maude et al., NEJM 2018292). These data suggest long lived CAR T cell persistence supports stand-alone therapy for ALL with durable responses.
Ghorashian:Celgene: Honoraria; novartis: Honoraria; UCLB: Patents & Royalties: UCLB. Kramer:UCLB: Patents & Royalties. Ciocarlie:Servier: Other: Financial Support. Farzaneh:Autolus Ltd: Equity Ownership, Research Funding. Pule:Autolus: Employment, Equity Ownership, Patents & Royalties. Amrolia:UCLB: Patents & Royalties.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal