

Abstract
Most patients with newly diagnosed multiple myeloma (MM) are aged > 65 years with 30% aged > 75 years. Many elderly patients are also vulnerable because of comorbidities that complicate the management of MM. The prevalence of MM is expected to rise over time because of an aging population. Most elderly patients with MM are ineligible for autologous transplantation, and the standard treatment has, until recently, been melphalan plus prednisone. The introduction of novel agents, such as thalidomide, bortezomib, and lenalidomide, has improved outcomes; however, elderly patients with MM are more susceptible to side effects and are often unable to tolerate full drug doses. For these patients, lower-dose-intensity regimens improve the safety profile and thus optimize treatment outcome. Further research into the best treatment strategies for vulnerable elderly patients is urgently needed. Appropriate screening for vulnerability and an assessment of cardiac, pulmonary, renal, hepatic, and neurologic functions, as well as age > 75 years, at the start of therapy allows treatment strategies to be individualized and drug doses to be tailored to improve tolerability and optimize efficacy. Similarly, occurrence of serious nonhematologic adverse events during treatment should be carefully taken into account to adjust doses and optimize outcomes.
Introduction
Multiple myeloma (MM) is a malignant disease characterized by uncontrolled plasma tumor cell proliferation, driven by intrinsic chromosomal abnormalities and extrinsic stromal cell support, together with the presence of monoclonal protein in the blood or urine or both.1,2 Typical clinical presentation at diagnosis includes anemia (commonly presenting as fatigue), skeletal lesions (presenting as bone pain), renal impairment, and hypercalcemia. In Western countries, the annual age-adjusted incidence of MM is 5.6 cases per 100 000 people. The median patient age at diagnosis is ∼ 70 years; only 37% of patients with newly diagnosed (ND) disease are aged < 65 years, 26% are aged 65-74 years, and 37% are aged ≥ 75 years.3 The annual prevalence of MM in patients aged 65-74 years is ∼ 31 cases per 100 000 people, and it increases to 46 cases per 100 000 people in patients aged ≥ 75 years. Furthermore, the number of elderly patients with MM will probably increase because of the improved survival times that are associated with novel agents coupled with the increasing life expectancy of the general population.
In recent years, the introduction of novel agents such as thalidomide, lenalidomide, and the proteasome inhibitor bortezomib, which are associated with high-dose therapy and autologous stem cell transplantation in young patients and standard chemotherapy in elderly patients, has changed the management of myeloma and extended overall survival (OS) times.4-7 An estimate of the 5-year relative survival of patients with MM in the United States from 1990-1992 to 2002-2004 reported a significant survival increase from 29%-35%. More substantial increases were seen in patients aged < 50 years (5-year relative survival from 45%-57%) and patients aged 50-59 years (5-year relative survival from 39%-48%). By contrast, increases were much less pronounced in patients aged 60-69 years (5-year relative survival from 31%-36%), and no improvement was seen in patients aged > 70 years (5-year relative survival from 27%-29%; Figure 1).3,5,6 Notably, similar results were observed, taking into account life expectancy with respect to age, sex, and era of diagnosis. In a large population-based cohort study on 14 381 patients with MM diagnosed in Sweden from 1973-2003, relative survival ratios, defined as the ratio of the observed survival divided by the expected survival, were computed as measures of survival. The 5-year relative survival ratios improved significantly over the time, but the improvement was confined to patients < 70 years.4

Five-year relative survival rates according to the year of diagnosis and the patients' age at diagnosis. Survival rates have increased over the past 35 years in all patient age groups, a trend attributed to the effect of novel agents such as thalidomide, bortezomib, and lenalidomide; however, significant increases in survival have only been observed in patients aged < 65 years at initial diagnosis.3
Five-year relative survival rates according to the year of diagnosis and the patients' age at diagnosis. Survival rates have increased over the past 35 years in all patient age groups, a trend attributed to the effect of novel agents such as thalidomide, bortezomib, and lenalidomide; however, significant increases in survival have only been observed in patients aged < 65 years at initial diagnosis.3
Many patients aged ≥ 75 years are vulnerable because of their comorbid conditions that complicate the presentation and management of MM. Personalized therapy using dose-adjusted regimens is, therefore, urgently needed for these patients. Vulnerable elderly patients are underrepresented in clinical trials,8 and this population is not well studied, despite that most MM diagnoses and related mortality occurs in persons aged > 65 years. Further research into the best treatment strategies for vulnerable elderly patients with MM is therefore required, including an improved definition of clinical vulnerability in the elderly. This review discusses the effect of age and vulnerability on outcomes in patients with MM, specifically focusing on the effect of these factors on treatment regimens in elderly patients.
Effect of age on MM prognosis and response to treatment
Aging is associated with an increased risk of developing malignancies, and most cancer diagnoses and deaths occur in people aged > 65 years.3 The global population is rapidly aging, and the number of persons aged ≥ 65 years is expected to double between 2000 and 2030. Cancer types for which the highest percentage increase in incidence is expected between 2010 and 2030 are stomach (67%), liver (59%), MM (57%), prostate (55%), pancreatic (55%), bladder (54%), lung (52%), and colorectal (52%).9
Myeloma biology may differ by age at presentation. Ludwig et al10 analyzed the associations between the presenting features and survival times in 1689 patients with NDMM aged < 50 years, compared with 8860 patients aged > 50 years. Younger patients were identified as having more favorable prognostic features, such as International Staging System and Durie-Salmon stages, and fewer adverse prognostic factors, including elevated C-reactive protein levels, low hemoglobin levels, increased serum creatinine levels, and poor performance status. Younger patients had a significantly longer median survival time than patients in the older cohort (5.2 years vs 3.7 years, respectively; P < .001). After adjusting for MM-unrelated mortality, lower International Staging System stage and other favorable prognostic features seem to account for the significantly longer survival of younger patients with MM.10
Several factors may underlie the effect of age on patient prognosis. The human aging process is associated with a gradual, progressive decrease in physiologic reserve. Changes in body composition occur with age (there is a reduction in muscle mass, an increase in body fat, and a reduction in intracellular water levels), and all these changes may affect drug metabolism and distribution, but are not considered to have a major effect on cancer therapies. More importantly, however, are the age-related changes that occur in organ function. Aging is associated with clinically significant reductions in renal function, gastric function, hepatic mass and blood flow, bone marrow status, and cardiovascular function.11-14 All of these changes may affect the pharmacokinetics and pharmacodynamics of drugs, altering clinical efficacy and potentially increasing toxicity. Age-related organ function and metabolic changes can, therefore, contribute to the poor tolerability of cancer treatments seen in elderly patients because of an increase in treatment-related adverse events (AEs). Reduced tolerability and reduced dose intensity lead to the poorer outcomes observed in elderly patients with cancer.
Effect of vulnerability on cancer outcome in elderly patients
Traditionally, the Karnofsky Performance Scale or the World Health Organization scores are used to determine the fitness of patients with cancer, but the role of performance status as unique marker of functional status needs to be revised. In elderly patients with or without cancer, 3 terms are commonly used interchangeably to describe vulnerable adults: frailty, comorbidity (or multiple chronic conditions), and disability. However, in geriatric medicine, there is a growing consensus that these are distinct clinical entities that are causally related. Frailty, comorbidity, and disability all occur individually and commonly among elderly patients, and each of these factors has clinical importance. Moreover, it is becoming increasingly clear that these 3 factors are interrelated and have a cumulative effect on the health and prognosis of elderly patients (Figure 2). The use of score tables established in geriatric medicine provides additional information to performance status: 9%-38% of elderly patients with good performance status (< 2) were partially or fully dependent on others to carry out ordinary activities, such as household tasks and personal care.15,16

The interrelation between the 3 components of vulnerability (comorbidity, frailty, and disability) and the main health care implications associated with each factor.
The interrelation between the 3 components of vulnerability (comorbidity, frailty, and disability) and the main health care implications associated with each factor.
Frailty
Frailty is a distinct entity recognized by clinicians, with many possible manifestations and no single symptom or sign that is itself sufficient or essential for a diagnosis.17 A phenotype of the clinically frail elderly adult has been defined, based on the presence of a critical mass of ≥ 3 core elements of frailty: weakness, poor endurance, weight loss, low physical activity, and slow gait speed. The presence of frailty has been identified as an independent predictor of disability and other adverse outcomes in elderly adults.18 The differing degrees of frailty are outlined in Table 1.
Levels of frailty and disability in elderly patients and related description
| Frailty grade | Description |
|---|---|
| Very fit | Active, energetic patients, who exercise regularly or occasionally |
| Moderately fit | Patients not regularly active beyond routinely walking |
| Vulnerable | Patients who can perform limited activities but yet do not need help from other people |
| Mildly frail | Patients who need help for household tasks (shopping, walking several blocks, managing their finances, and medications) |
| Moderately frail | Patients who need partial help for their personal care (dressing, bathing, toileting, eating) |
| Severely frail | Patients completely dependent on other people for their personal care |
| Frailty grade | Description |
|---|---|
| Very fit | Active, energetic patients, who exercise regularly or occasionally |
| Moderately fit | Patients not regularly active beyond routinely walking |
| Vulnerable | Patients who can perform limited activities but yet do not need help from other people |
| Mildly frail | Patients who need help for household tasks (shopping, walking several blocks, managing their finances, and medications) |
| Moderately frail | Patients who need partial help for their personal care (dressing, bathing, toileting, eating) |
| Severely frail | Patients completely dependent on other people for their personal care |
Comorbidity
The formal definition of comorbidity is the concurrent presence of ≥ 2 medically diagnosed diseases in the same person, with the diagnosis of each contributing disease based on established, widely recognized criteria.17 Many prognostic indices for the elderly that incorporate age or comorbidity or both are available19-21 ; the Charlson comorbidity index is the one most frequently used in patients with cancer.19,22 However, this is complex, and a more simple score index for comorbidities in MM is needed. The Charlson index is a summary measure of 19 comorbid conditions weighted 1-6 corresponding to disease severity. This gives a total score ranging from 0 to 37. It can be adapted to account for increasing age, adding 1 point to the score for each decade older than the age of 50 years. With this index, the relative risk of death that can be attributed to an increase of 1 point in the comorbidity score is equivalent to an additional decade of age.19 With aging, the incidence of comorbid conditions increases markedly, largely because the frequency of individual chronic conditions rises with age. As a result, 35% of men and 45% of women aged 60-69 years in the United States have ≥ 2 comorbid conditions; this percentage increases dramatically to 53% of men and 70% of women by age 80 years.23 Comorbidity is associated with polymedication and increased risk of drug interactions.
Disability
Disability (which can include both physical and mental impairments or limitations) can be defined as difficulty or dependency in carrying out activities essential to independent living, including both essential personal care and household tasks, and activities that are important to maintain a person's quality of life.24,25 Physical disability is common among elderly adults and is more common in elderly women than men. The main causes of physical disability in the elderly are chronic diseases such as cardiovascular disease, stroke, arthritis, and, in patients with myeloma, orthopedic problems plus pain,26 highlighting the interrelation between disability and comorbidity. The incidence of disability rises steadily with age among those aged ≥ 65 years.25 Of community-dwelling adults, 20%-30% of those aged > 70 years report some disability in mobility, tasks essential to household management (eg, shopping, meal preparation, managing money), and basic self-care tasks (eg, washing, dressing, eating). Disability, independent of its causes, is associated with a higher risk of mortality27 ; disabled adults are more likely to become hospitalized.26,28
Effect of comorbidity on cancer outcomes
No data are currently available on the effect of vulnerability on outcomes in patients with MM, but the issues relating to comorbidity and cancer treatment are discussed in the following section in relation to elderly patients with cancer in general.
An observational cohort study of 17 712 patients receiving treatment for multiple cancer types suggested that the severity of comorbidities affected survival outcomes in a progressive manner, independent of cancer stage.29 This observation was supported by several studies in which comorbidities were associated with a higher risk of mortality.30-35
Comorbid conditions have rarely been systematically studied among hematologic patients. However, a large population-based study of 1708 patients with myelodysplastic syndromes (MDSs) showed that those patients with MDS and comorbid conditions had a significantly higher risk of death than patients without comorbidities. The risk was found to increase with an increasing number of comorbid conditions and, therefore, a higher Charlson score (hazard ratio [HR] for death = 1.19 for patients with a Charlson index of 1-2; and HR = 1.77 for patients with a Charlson index ≥ 3).36 Wang et al also reported that patients with MDS with congestive heart failure or chronic obstructive pulmonary disease have significantly shorter survival times than their counterparts without those conditions,36 whereas diabetes does not appear to have an effect on survival in patients with MDS. Another study involving 998 elderly patients with acute leukemia or MDS supported these findings on the effect of comorbidity and identified several factors associated with poor outcome, including age ≥ 75 years, a longer duration of prior hematologic disorder, and abnormal organ function.37
Relation between age and vulnerability in MM
Although there is evidence for the separate prognostic importance of age, comorbidity, frailty, and disability for health outcomes, it is also important to note that many patients have ≥ 2 of these factors, and that this has a cumulative, adverse effects on their prognosis. The frequently used Charlson index has been described earlier, but another prognostic index has also been successfully developed for assessment of mortality risk after hospitalization in elderly patients aged > 70 years. This uses the combined effect of age, physical disability (determined by levels of dependency in activities in daily living), and levels of comorbidity.20
Studies in geriatric oncology populations, including patients with prostate, lung, and ovarian cancers, have also shown the combined effects of age, comorbidity, frailty, and disability on patient prognosis.38-40 In a large prospective trial involving 427 patients with cancer (more than one-half of whom had hematologic malignancies), age, severe comorbidities, functional impairment, and tumor type were all found to be independently related to shorter survival times.41 Similarly, in the setting of colorectal carcinoma, a model developed as part of a Surveillance, Epidemiology, and End Results registry review used comorbidity and age in addition to sex and disease stage in a model to predict early mortality.33 The number of comorbid conditions a patient had was found to significantly predict early mortality.
In hematologic oncology, data on the combined effect of vulnerability and age are limited. As discussed earlier, a series of patients with MDS aged ≥ 66 years identified comorbidity (assessed with the Charlson comorbidity index) as a significant predictor of mortality. A comorbidity index developed specifically for patients undergoing hematopoietic cell transplantation was found to have high sensitivity and was effective in predicting outcomes in patients with acute myeloid leukemia.42 A retrospective analysis of 968 adults with acute myeloid leukemia was designed to assess the biology of the condition change with patient age. In this analysis, elderly patients presented more frequently with poorer performance status and with unfavorable cytogenetics. In particular, the combination of poor performance status and advanced age identified a group of patients who were highly probable to die within 30 days of starting induction therapy.43 Unfortunately, however, similar data addressing the prognostic effect of age and vulnerability in patients with MM are not currently available.
Clinical treatment of elderly patients with MM
Standard treatment regimens for ND elderly patients (≥ 65 years)
Patients with NDMM aged > 65 years are generally considered ineligible for autologous stem cell transplantation because they are physically unable to withstand toxicity of the procedure, although this considerably differs from patient to patient, and melphalan dose reduction may allow even patients > 70 years to undergo transplantation. Standard frontline treatment for elderly, transplantation-ineligible patients has, until recently, been the alkylating agent melphalan in combination with prednisone (MP). This regimen is well tolerated in vulnerable elderly patients and is associated with good response rates and survival outcomes that are comparable with other conventional combinations of chemotherapy.44,45 However, the availability of novel agents, including the immunomodulatory agents thalidomide and lenalidomide, and the proteasome inhibitor bortezomib, has led to the development of new treatment options for patients with NDMM.46 These novel agents can be used in combination with MP as well as in other treatment combinations, such as lenalidomide with low-dose dexamethasone.47-51
MP versus combination melphalan, prednisone, and thalidomide
Six randomized studies have compared the efficacy and safety of the standard MP regimen with the new combination of MP plus thalidomide (MPT).48-50,52-55 Those studies reported improved clinical response rates and a longer progression-free survival (PFS) associated with MPT compared with MP, but the effect of MPT on OS was unclear (Table 2).47-58 However, a recent meta-analysis of data from 1682 patients in the 6 randomized studies of MPT versus MP has confirmed a significant improvement in PFS and a trend toward significant improvement in OS when thalidomide is added to MP as a frontline treatment in elderly patients with NDMM.59 MPT was associated with better 1-year overall response rate (ORR; 59% with MPT vs 37% with MP) and prolonged PFS (median, 20 months with MPT vs 15 months with MP; P < .0001). The thalidomide regimen also led to a 17% risk reduction of death compared with MP (HR = 0.83; 95% confidence interval, 0.73-0.94; P = .004) and an increased median OS time of 6.6 months.59 This improvement was less pronounced in patients aged ≥ 75 years. In the Nordic study, the median PFS of these patients was shorter than for patients aged 65-74 years (10 months with MPT vs 6 months with MP), and no improvement was observed in OS.52 Similar results have been reported in the Myeloma IX study that used thalidomide in combination with the alternative alkylating agent, cyclophosphamide, and steroid, dexamethasone.60
Outcomes from randomized phase 3 clinical trials of different treatment regimens in elderly patients with NDMM
| Regimen | Median age, y | Dosing | CR rate, % | Median PFS, mo | Median OS, mo | Discontinuation rate, % | Nonhematologic grade 3-4 AEs, % |
|---|---|---|---|---|---|---|---|
| MPT48 | 69 | M: 0.25 mg/kg on days 1-4 for twelve 6-wk cycles P: 40 mg/m2 on days 1-4 for twelve 6-wk cycles T: 400 mg/d for twelve 6-wk cycles | 13 | 28 | 52 | 45 | 42 |
| MPT49,50 | 72 | M: 4 mg/m2 on days 1-7 for six 4-wk cycles P: 40 mg/m2 on days 1-7 for six 4-wk cycles T: 100 mg/d until relapse | 16 | 22 | 45 | 34 | 55* |
| MPT52 | 72 | M: 0.25 mg/kg on days 1-5 for eight 4-wk cycles P: 1 mg/kg on days 1-5 for eight 4-wk cycles T: 200 mg/d for eight 4-wk cycles, followed by 50 mg/d until relapse | 23† | 13‡ | 40 | 36 | 50 |
| MPT53 | 78 | M: 0.2 mg/kg on days 1-4 for twelve 6-wk cycles P: 2 mg/kg on days 1-4 for twelve 6-wk cycles T: 100 mg/d for twelve 6-wk cycles | 7 | 24 | 44 | 42 | NA |
| MPT54 | 74 | M: 0.25 mg/kg on days 1-4 for 6-wk cycles until plateau P: 100 mg/d on days 1-4 for 6-wk cycles until plateau T: 400 mg/d until plateau, reduced to 200 mg/d until progression | 13 | 15 | 29 | 32 | 40 |
| MPT55 | 69 | M: 9 mg/m2 on days 1-4 for eight 6-wk cycles P: 60 mg/m2 on days 1-4 for eight 6-wk cycles T: 100 mg/d for eight 6-wk cycles, followed by100 mg/d until relapse | 9 | 21§ | 26 | 16 | NA |
| VMP47,56 | 71 | V: 1.3 mg/m2 on days 1, 4, 8, 11, 22, 25, 29, and 32 for first four 6-wk cycles; days 1, 8, 15, and 22 for subsequent five 6-wk cycles M: 9 mg/m2 on days 1-4 for five 6-wk cycles P: 60 mg/m2 on days 1-4 for five 6-wk cycles | 30 | NA | Not reached | 34 | 91* |
| VMP57 | 71 | V: 1.3 mg/m2 on days 1, 8, 15, and 22 for nine 5-wk cycles M: 9 mg/m2 on days 1-4 for nine 5-wk cycles P: 60 mg/m2 on days 1-4 for nine 5-wk cycles | 24 | 23 | Not reached | 17 | 33 |
| MPR-R58 | NA | M: 0.18 mg/kg on days 1-4 for nine 4-wk cycles P: 2 mg/kg on days 1-4 for nine 4-wk cycles R: 10 mg on days 1-21 for nine 4-wk cycles R: 10 mg/d until relapse | 16 | 31 | Not reached | 14¶ | NA |
| Rd51 | 66 | R: 25 mg on days 1-21 d: 40 mg on days 1, 8, 15, 22 in 4-wk cycles | 4 | 25 | Not reached | 19 | NA |
| VMPT57 | 71 | V: 1.3 mg/m2 on days 1, 8, 15, and 22 for nine 5-wk cycles and on days 1, 15 until relapse M: 9 mg/m2 on days 1-4 for nine 5-wk cycles P: 60 mg/m2 on days 1-4 for nine 5-wk cycles T: 50 mg daily until relapse | 38 | Not reached | Not reached | 23 | 46 |
| Regimen | Median age, y | Dosing | CR rate, % | Median PFS, mo | Median OS, mo | Discontinuation rate, % | Nonhematologic grade 3-4 AEs, % |
|---|---|---|---|---|---|---|---|
| MPT48 | 69 | M: 0.25 mg/kg on days 1-4 for twelve 6-wk cycles P: 40 mg/m2 on days 1-4 for twelve 6-wk cycles T: 400 mg/d for twelve 6-wk cycles | 13 | 28 | 52 | 45 | 42 |
| MPT49,50 | 72 | M: 4 mg/m2 on days 1-7 for six 4-wk cycles P: 40 mg/m2 on days 1-7 for six 4-wk cycles T: 100 mg/d until relapse | 16 | 22 | 45 | 34 | 55* |
| MPT52 | 72 | M: 0.25 mg/kg on days 1-5 for eight 4-wk cycles P: 1 mg/kg on days 1-5 for eight 4-wk cycles T: 200 mg/d for eight 4-wk cycles, followed by 50 mg/d until relapse | 23† | 13‡ | 40 | 36 | 50 |
| MPT53 | 78 | M: 0.2 mg/kg on days 1-4 for twelve 6-wk cycles P: 2 mg/kg on days 1-4 for twelve 6-wk cycles T: 100 mg/d for twelve 6-wk cycles | 7 | 24 | 44 | 42 | NA |
| MPT54 | 74 | M: 0.25 mg/kg on days 1-4 for 6-wk cycles until plateau P: 100 mg/d on days 1-4 for 6-wk cycles until plateau T: 400 mg/d until plateau, reduced to 200 mg/d until progression | 13 | 15 | 29 | 32 | 40 |
| MPT55 | 69 | M: 9 mg/m2 on days 1-4 for eight 6-wk cycles P: 60 mg/m2 on days 1-4 for eight 6-wk cycles T: 100 mg/d for eight 6-wk cycles, followed by100 mg/d until relapse | 9 | 21§ | 26 | 16 | NA |
| VMP47,56 | 71 | V: 1.3 mg/m2 on days 1, 4, 8, 11, 22, 25, 29, and 32 for first four 6-wk cycles; days 1, 8, 15, and 22 for subsequent five 6-wk cycles M: 9 mg/m2 on days 1-4 for five 6-wk cycles P: 60 mg/m2 on days 1-4 for five 6-wk cycles | 30 | NA | Not reached | 34 | 91* |
| VMP57 | 71 | V: 1.3 mg/m2 on days 1, 8, 15, and 22 for nine 5-wk cycles M: 9 mg/m2 on days 1-4 for nine 5-wk cycles P: 60 mg/m2 on days 1-4 for nine 5-wk cycles | 24 | 23 | Not reached | 17 | 33 |
| MPR-R58 | NA | M: 0.18 mg/kg on days 1-4 for nine 4-wk cycles P: 2 mg/kg on days 1-4 for nine 4-wk cycles R: 10 mg on days 1-21 for nine 4-wk cycles R: 10 mg/d until relapse | 16 | 31 | Not reached | 14¶ | NA |
| Rd51 | 66 | R: 25 mg on days 1-21 d: 40 mg on days 1, 8, 15, 22 in 4-wk cycles | 4 | 25 | Not reached | 19 | NA |
| VMPT57 | 71 | V: 1.3 mg/m2 on days 1, 8, 15, and 22 for nine 5-wk cycles and on days 1, 15 until relapse M: 9 mg/m2 on days 1-4 for nine 5-wk cycles P: 60 mg/m2 on days 1-4 for nine 5-wk cycles T: 50 mg daily until relapse | 38 | Not reached | Not reached | 23 | 46 |
CR indicates complete response; PFS, progression-free survival; OS, overall survival; AE, adverse event; MPR-R, melphalan, prednisone, and lenalidomide followed by lenalidomide maintenance; NA, not available; Rd, lenalidomide plus low-dose dexamethasone; VMP, bortezomib, melphalan, and prednisone; and VMPT, bortezomib, melphalan, prednisone, and thalidomide.
Both hematologic and nonhematologic AEs.
CR plus very good partial response (CR alone not available).
Event-free survival.
Disease-free survival.
Includes both patients who received lenalidomide maintenance and those who did not.
The most common grade 3-4 nonhematologic AEs associated with MPT were peripheral neuropathy (6%-23%), thromboembolism (3%-12%), infections (10%-13%), cardiac complications (2%-7%), and gastrointestinal events (∼ 5%). Thalidomide discontinuation because of AEs varied from 33%-45%.61 Some studies reported a doubling of early toxic deaths among patients aged ≥ 75 years and no favorable effect of thalidomide on OS in patients with higher World Health Organization performance status.52,54
MP versus combination bortezomib, melphalan, and prednisone
Bortezomib is effective and well tolerated in patients with relapsed or refractory MM.62,63 The clinical value of adding bortezomib to the standard MP regimen (VMP) was explored in the Velcade as Initial Standard Therapy (VISTA) study.47,56 ORR in patients treated with VMP was higher than with the MP regimen (80% vs 56%, respectively; P < .001). Similarly, a higher proportion of these patients achieved a complete response compared with the MP regimen (30% vs 4%, respectively; P < .001); time to progression was also prolonged (24 vs 16.6 months, respectively; P < .001). Importantly, OS was significantly extended in the VMP regimen (HR = 0.61; P = .008).47 These results have been confirmed by an extended follow-up of the VISTA study. After a median follow-up of 36.7 months the risk of death associated with the VMP regimen was 35% lower than with MP (HR = 0.653; P < .001). Median survival time was not reached in the VMP regimen compared with 43 months in the MP regimen.56 In addition in the VISTA study, outcomes were worse in patients aged ≥ 75 years; within the VMP group, the 3-year OS was longer among patients aged < 75 years (74%) than for patients aged ≥ 75 years (55%).56 Similar results both for efficacy and safety were observed in a US community-based phase 3b study that compared VMP with bortezomib-dexamethasone and with bortezomib-thalidomide-dexamethasone.64
The incidence of any grade 3-4 hematologic and nonhematologic AEs with VMP was 91%, leading to a bortezomib discontinuation rate of 34%. Neutropenia (40%) is the main AE associated with VMP, followed by thrombocytopenia (37%), peripheral neuropathy (14%), infections (10%), and gastrointestinal events (7%).47,56 The recent update of the VISTA study showed that the rate of severe AEs was higher in the first 4 cycles when a twice-weekly bortezomib schedule was administered; it was lower during the last 5 cycles when the lower-dose intensity once-weekly bortezomib schedule was administered.56 Two subsequent studies showed that a once-weekly schedule significantly reduced the incidence of any grade 3-4 hematologic and nonhematologic AEs, in particular peripheral neuropathy (7%-8%), as well as the rate of discontinuation because of toxicity.65,66 This improvement in safety was obtained without negatively affecting outcomes because, although the cumulative planned dose was lower in the once-weekly group (46.8 vs 67.6 mg/m2), the cumulative delivered dose of bortezomib was similar in the 2 groups (39.4 mg/m2 in the once-weekly group and 40.1 mg/m2 in the twice-weekly group; Table 3).47,51,57,65,66
Outcome of patients with ND disease treated with full-dose or reduced-dose regimens
| Any grade 3-4 AEs, % | Discontinuation rate because of toxicity, % | PFS, % | OS, % | |
|---|---|---|---|---|
| Standard dose therapies | ||||
| VMP47 | 91 | 3 | 50 at 2 y | 68 at 3 y |
| RD51 | 52 | 27 | 48 at 2 y | 78 at 2 y |
| Lower dose therapies | ||||
| VMP57,65 | 51 | 12-17 | 46-50 at 3 y | 74-87 at 3 y |
| Rd51 | 35 | 19 | 52 at 2 y | 88 at 2 y |
| Any grade 3-4 AEs, % | Discontinuation rate because of toxicity, % | PFS, % | OS, % | |
|---|---|---|---|---|
| Standard dose therapies | ||||
| VMP47 | 91 | 3 | 50 at 2 y | 68 at 3 y |
| RD51 | 52 | 27 | 48 at 2 y | 78 at 2 y |
| Lower dose therapies | ||||
| VMP57,65 | 51 | 12-17 | 46-50 at 3 y | 74-87 at 3 y |
| Rd51 | 35 | 19 | 52 at 2 y | 88 at 2 y |
AE indicates adverse event; PFS, progression-free survival; OS, overall survival; RD lenalidomide plus high-dose dexamethasone; and Rd, lenalidomide plus low-dose dexamethasone.
MP versus combination melphalan, prednisone, and lenalidomide followed by continuous lenalidomide treatment
The immunomodulatory derivative of thalidomide compound lenalidomide has shown efficacy in patients with relapsed or refractory MM,67,68 and it has also been evaluated in combination with MP as a frontline treatment for patients with NDMM.58
Initial results of the randomized trial that compared the addition of lenalidomide with MP followed by lenalidomide maintenance treatment (MPR-R) with standard MP (MM-015 study) indicate that MPR-R was superior to the standard MP regimen.58 The ORR was significantly higher with MPR-R than with MP (77% vs 50%, respectively; P < .001). Complete response rates were also significantly higher with MPR combination therapy (16% vs 4%; P < .001). After a median follow-up of 21 months, MPR-R led to gains on PFS and reduced the risk of disease progression by 58% compared with MP alone (HR = 0.423; P < .001). Median PFS was 31 months in the MPR-R regimen compared with 14 months for MPR and 13 months for MP, the 2-year PFS was significantly higher in patients who received lenalidomide continuous therapy than for fixed-duration MP (55% vs 16%, respectively; P < .001). The importance of continuous lenalidomide therapy on outcomes is elucidated by a landmark analysis of PFS in patients completing induction therapy and proceeding onto maintenance therapy. This showed a 75% reduced risk of disease progression with continuous lenalidomide therapy versus no treatment (HR = 0.245; 95% confidence interval, 0.126-0.476; P < .001). However, no differences in OS have been reported, probably because of the short duration of follow-up to date, the administration of lenalidomide at relapse, and possibly more resistant relapses.58 Preliminary analysis indicates that outcomes may be worse in patients aged ≥ 75 years, possibly explained by the lower relative dose intensity of MPR that these patients received during induction therapy. In patients aged 65-74 years, MPR alone was superior to MP in terms of PFS (HR = 0.675; P = .030), but this advantage was not evident in patients aged ≥ 75 years. Hence, the MPR toxicity profile was excessive for frail patients and negatively affected efficacy. The main grade 3-4 hematologic and nonhematologic AEs associated with MPR were neutropenia (52%-71%), thrombocytopenia (23%-38%), infections (10%), and thromboembolism (5%).58,69 In the first 9 cycles of therapy, the discontinuation rate because of AEs was 4% in the MP group among patients aged 65-74 years and 8% in patients aged ≥ 75 years. The discontinuation rate because of toxicity was 12% in the MPR or MPR-R group among patients aged 65-74 years, and 19% in patients aged ≥ 75 years. The cumulative dose intensity was similar in MP and MPR or MPR-R treatment for patients aged 65-74 years (97% and 88%, respectively), whereas it was reduced in patients aged ≥ 75 years (97% and 56%, respectively).58 These data clearly show that the intended dose intensity is well maintained in the MP group, is adequate for the MPR regimens in patients aged 65-74 years, and is totally unmaintained in patients aged ≥ 75 years. Thus, further dose reduction to keep the patient on therapy is needed.
Lenalidomide and dexamethasone
In patients with NDMM, lenalidomide in combination with high-dose dexamethasone (RD) has been shown to improve PFS and ORR rates compared with high-dose dexamethasone monotherapy.70 However, RD was associated with an increased incidence of thromboembolic complications, so an adapted regimen of lenalidomide with low-dose dexamethasone (Rd) was evaluated.51 ORR was lower with Rd (70%) than with RD (81%). The higher response rates for the high-dose dexamethasone regimen did not translate into superior PFS (median, 25.3 months in the Rd group vs 19.1 months in the RD group). The Rd regimen was associated with significantly improved 1-year OS than with RD (96% vs 87%, respectively; P = .0002), and treatment-related toxicity was also significantly reduced. Similar results were observed when the analysis was restricted to 248 patients who did not receive transplant.51
These data indicate that the Rd regimen is an effective regimen for patients with ND disease with acceptable toxicity. Although the advantages associated with Rd compared with RD were also confirmed in a subgroup of patients aged > 70 years, inferior outcomes were observed in this subset of patients; the ORR was 74% with Rd and 75% with RD. Median PFS was 22 months in the low-dose dexamethasone group compared with 16 months in the high-dose group, and OS was improved in the low-dose dexamethasone regimen (3-year OS, 73% in the Rd group vs 61% in the RD group).71
The incidence of any grade 3-4 nonhematologic AEs was 35% with Rd and 52% with RD, and the respective discontinuation rate because of AEs was 19% and 27%, respectively. Deep vein thrombosis and pulmonary embolism were the most frequent toxicities and were reported in 12% of patients in the Rd group and 26% in the RD group; infection was another common AE (9% with Rd and 16% with RD).51 The advantages of Rd over RD were more pronounced in patients aged > 70 years because of the poor tolerability, higher toxicity profile, and higher mortality rate associated with the high-dose dexamethasone in this population. In these patients, the incidence of any grade 3-4 nonhematologic AE increased to 59% in the Rd regimen and 78% in the RD regimen.71 A phase 2 trial in relapsed/refractory patients showed that lower doses of lenalidomide (15 mg) plus low-dose dexamethasone (40 mg weekly) significantly reduced the incidence of hematologic toxicities (from 15%-30% to 2%-13%), infections (from 20% to 8%), and thromboembolism (from 20% to 5%).72
Evidence is now emerging that maintenance/continuous therapy with novel agents such as thalidomide,73-75 lenalidomide,58,76,77 or bortezomib57,65 is improving PFS with a potential to improve OS. However, in elderly patients it is particularly important to start treatment at a dose that can be tolerated over the long term.
Tolerability of novel antimyeloma treatment in elderly patients
Although the novel agents offer important improvements in survival for patients with MM, the incidence of grade 3-4 AEs are significantly higher with combination regimens that are based on novel agents than with traditional chemotherapy regimens (Table 3). This is reflected in the discontinuation rates because of AEs in regimens containing novel agents (13%-45% across studies). Elderly patients with MM are more susceptible to AEs associated with treatments, with 42%-53% of elderly patients experiencing grade 3-4 AEs in the early cycles of treatment with a novel agent.48-50,52,78
Drug-related treatment complications are prevalent among elderly or vulnerable patients with MM and may lead to premature treatment discontinuations or lower dose intensities. Therefore, to maintain treatment efficacy it is crucial that these are anticipated and managed accordingly. This highlights the need for dosing strategies to improve the tolerability of treatment with the novel antimyeloma agents, especially during induction therapy, in vulnerable, elderly patients to allow for long-term treatment. Furthermore, the tolerability of treatment could be improved with supportive therapy, particularly in elderly patients. G-CSFs decrease or prevent neutropenia. Aspirin or low-molecular-weight heparins should be used to decrease the risk of thromboembolic events when immunomodulatory compounds are given. Erythropoiesis-stimulating agents can be used to treat chemotherapy-associated anemia with iron supplements improving the effectiveness of treatment. Bone pain requires systemic analgesia, local measures, and chemotherapy. Local radiotherapy is effective for palliation of bone pain, and bisphosphonates can reduce new bone lesions, pathologic fractures, and hypercalcemia. Appropriate hydration, urine alkalinization, rapidly acting therapy for myeloma, and treatment of hypercalcemia, hyperuricemia, and infections prevent further deterioration of renal function in patients with renal impairment.
In the context of treatment tolerability and individualized treatment strategies, it is also important to consider the management of elderly patients with MM with relapsed or with relapsed and refractory disease. These patients are exposed to multiple sequential lines of treatment, which probably have a progressive weakening effect on their overall physical condition. Therefore, treatment strategies for elderly patients should have minimal cumulative toxicity across the lines of treatment. These should not exacerbate any preexisting conditions such as peripheral neuropathy, which commonly develops as an adverse effect of treatment with thalidomide or bortezomib. Supportive therapies, dose adjustments, clinical vigilance, and patient education are important to minimize AEs and maintain compliance with antimyeloma treatment.
Tailored therapy for the treatment of elderly patients with MM
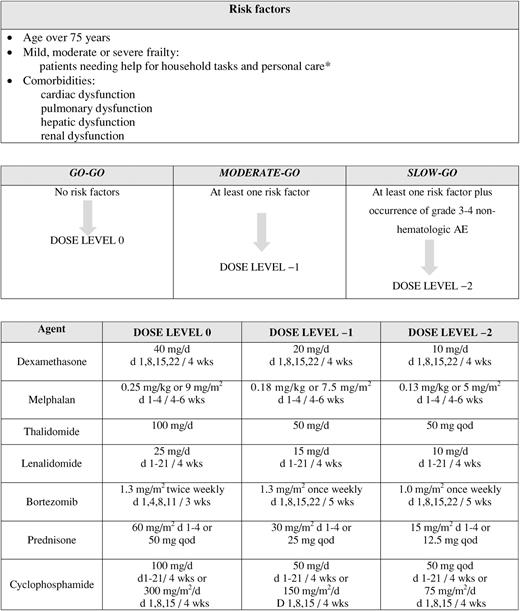
The age-related changes in physiology combined with comorbid conditions, disability, or frailty have important implications for the treatment of patients with cancer. However, in patients with MM treatment should not be withheld solely on the basis of age. A patient's overall physical condition and organ function should be assessed to determine his or her ability to tolerate treatment. Elderly patients with NDMM should, therefore, be assessed for frailty, comorbidity, and disability. Cardiac performance, pulmonary and hepatic functions, renal function (especially in elderly patients determined with creatinine clearance), and peripheral neuropathy should be evaluated. On the basis of the results of these tests it is possible to stratify patients into those suitable for full-dose therapy or combination drug treatment and those requiring adjusted-dose treatment strategies (Table 4). We propose recommendations whereby patients with ≥ 1 risk factor (age ≥ 75 years, frailty, comorbidities, disability, or grade 3-4 nonhematologic AEs) should be considered for a reduced-dose treatment strategy. Patients without risk factors should be administered full-dose treatment.46,79 Recommended starting doses and dose adjustments according to age groups and vulnerability status are presented in Table 4. When a grade 3 or 4 AE occurs during treatment, therapy should be discontinued until the toxicity has resolved, usually by the start of the next cycle, at which point treatment can be restarted at a lower dose (Table 4). Modifying drug doses at the start of treatment or to manage AEs is important because it improves tolerability. Treatment should be interrupted and changed in patients not responding after ≥ 3 cycles, whereas continuous long-term therapy beyond best response may be important for sustained disease control of the residual disease in MM.57,58,65
Conclusions
Advanced age and patient vulnerability have a significant and cumulative effect on survival outcomes and treatment efficacy in patients with cancer. In MM, elderly patients have a worse prognosis from initial diagnosis than patients aged < 65 years. Currently, the improvements in survival associated with the novel antimyeloma agents have not been observed in elderly patients.
No data are available that assess screening for vulnerability before choosing and starting therapy for MM. However, although no data are available specifically for patients with MM because of the underrepresentation in clinical trials of elderly adults and patients with comorbidities, it is reasonable to translate data on elderly general population to the MM population. We can, therefore, speculate that the continued poor prognosis of elderly patients with MM may be attributable, at least in part, to physical vulnerability and the effect that this has on patients' ability to tolerate complex treatment regimens. It is, therefore, important to consider the age, physical condition, and comorbidity status for all elderly patients with MM when planning treatment. Appropriate dose adjustments or use of modified treatment regimens should be made accordingly to improve the tolerability of treatment. Well-tolerated regimens will probably reduce the need for treatment interruptions and thereby should optimize treatment efficacy.
Future trials should address the role of age, comorbidities, and geriatric assessment by stratifying patients with MM into treatment groups at different risk of mortality. In addition to greater inclusion of vulnerable elderly patients in standard trial protocols, trials that address specific needs in elderly adults (eg, renal impairment) may also yield important insights. To promote the enrollment of elderly adults in clinical trials it may be necessary to relax standard protocol eligibility criteria by focusing on developing therapeutics suitable for patients with comorbid conditions. Clinical trials focused on optimizing MM treatment regimens for both fit and unfit elderly adults are urgently needed. The data from such trials, when available, will eventually lead to tailored, “personalized” therapy for elderly patients with MM and thereby improve OS in this large patient group.
Acknowledgments
The authors thank editorial assistant Giorgio Schirripa.
Authorship
Contribution: All authors developed the consensus, provided critical review and edits to the manuscript, gave approval to the final manuscript, and significantly participated in the development of the consensus and writing of the manuscript.
Conflict-of-interest disclosure: A.P. has received honoraria from Celgene, Janssen-Cilag, Merck, and Amgen and served on the advisory board for Celgene and Janssen-Cilag; S.B. has received honoraria from Celgene, Janssen-Cilag, and Novartis, and served on the advisory committee of Merck Sharp & Dohme; H.L. has received honoraria from and served on the advisory board for Celgene and speakers bureau for Celgene and Ortho-Biotech; M.A.D. has received honoraria from Ortho-Biotech, Celgene, and Novartis; J.B. has received honoraria from Celgene and Janssen-Cilag; M.V.M. has received honoraria from Celgene, Janssen-Cilag, Millennium, and Novartis; L.R. has received honoraria from Celgene and Janssen-Cilag; M. Boccadoro has received research support from and served on the consultancy and the scientific advisory board for Celgene and Janssen-Cilag; M.C. has received honoraria and served on speakers' bureaux for Janssen-Cilag, Millennium Pharmaceuticals, Celgene, and Novartis and has been a consultant for Janssen-Cilag and Millennium Pharmaceuticals; H.L. has been a consultant for Celgene and Genmab; S.Z. has received honoraria from and served on the advisory board for Celgene and Janssen-Cilag; E.T. has received honoraria from and served on the advisory board for Novartis, Amgen, Celgene, and Janssen-Cilag; F.D. has served on the advisory board for Celgene, Novartis, and Ortho-Biotech and received travel support from Celgene and Ortho-Biotech; P.G. served as chairman of data safety and on the monitoring committee for BioInvent and served on the speakers bureau for Celgene, Nordic Cancer Union, Amgen, Janssen-Cilag, and Nordpharma; R.H. has received honoraria from Celgene, Janssen-Cilag, and MDS, and educational grants from Celgene, Janssen-Cilag; F.L.D.C. has been a consultant and received honoraria from Celgene, Janssen-Cilag, Merck Sharp & Dohme, and OM Pharma; O.S. has received honoraria from Celgene, Janssen-Cilag, Amgen, and Novartis, and research funding from Janssen-Cilag and Novartis; M. Beksac has received honoraria from Celgene and Janssen-Cilag; G.M. has been a consultant and served on the advisory board for Celgene, Johnson & Johnson, and Lilly; H.E. has served on the advisory board for Celgene, Novartis, and Janssen-Cilag; J.F.S.M. has served on the advisory board for Millennium, Celgene, and Johnson & Johnson; P.S. has received research support from Celgene, Janssen-Cilag, and Onyx, and served on the advisory board for Celgene, Janssen-Cilag, Millennium, and Onyx. The remaining authors declare no competing financial interests.
Correspondence: Antonio Palumbo, Myeloma Unit, Division of Hematology, University of Torino, AOU S. Giovanni Battista, Torino, Italy; e-mail: appalumbo@yahoo.com.
