

Key Points
The UKALL-CNA classifier is a validated and robust prognostic tool that can be deployed in a variety of clinical trial settings.
The UKALL-CNA classifier can be used to refine risk stratification for patients with intermediate-risk cytogenetics.

Abstract
Genetic abnormalities provide vital diagnostic and prognostic information in pediatric acute lymphoblastic leukemia (ALL) and are increasingly used to assign patients to risk groups. We recently proposed a novel classifier based on the copy-number alteration (CNA) profile of the 8 most commonly deleted genes in B-cell precursor ALL. This classifier defined 3 CNA subgroups in consecutive UK trials and was able to discriminate patients with intermediate-risk cytogenetics. In this study, we sought to validate the United Kingdom ALL (UKALL)–CNA classifier and reevaluate the interaction with cytogenetic risk groups using individual patient data from 3239 cases collected from 12 groups within the International BFM Study Group. The classifier was validated and defined 3 risk groups with distinct event-free survival (EFS) rates: good (88%), intermediate (76%), and poor (68%) (P < .001). There was no evidence of heterogeneity, even within trials that used minimal residual disease to guide therapy. By integrating CNA and cytogenetic data, we replicated our original key observation that patients with intermediate-risk cytogenetics can be stratified into 2 prognostic subgroups. Group A had an EFS rate of 86% (similar to patients with good-risk cytogenetics), while group B patients had a significantly inferior rate (73%, P < .001). Finally, we revised the overall genetic classification by defining 4 risk groups with distinct EFS rates: very good (91%), good (81%), intermediate (73%), and poor (54%), P < .001. In conclusion, the UKALL-CNA classifier is a robust prognostic tool that can be deployed in different trial settings and used to refine established cytogenetic risk groups.
Introduction
Acute lymphoblastic leukemia (ALL) is the most common type of cancer in childhood. Survival rates in high-income countries have improved from 10% in the 1960s to 90% in 2015.1 Although similar improvements have been achieved in middle-income countries, the absolute survival rates are lower (∼75%).2 Treatment stratification according to biological features and response has played an important role in the improvement of survival rates. Despite these improvements relapse remains the major clinical challenge in ALL. Therefore, it is crucial to develop novel risk-stratification algorithms to help ensure that each patient receives the appropriate type and intensity of treatment to further increase survival rates and reduce long-term side effects.
Chromosomal abnormalities are the hallmark of ALL and have been widely used as prognostic markers. For example, in B-cell precursor ALL (BCP-ALL), patients with high hyperdiploidy (51-65 chromosomes) or ETV6-RUNX1 have a favorable outcome,3 while patients with BCR-ABL1, KMT2A (MLL) rearrangements, TCF3-HLF, intrachromosomal amplification of chromosome 21 (iAMP21), near haploidy (<30 chromosomes), or low hypodiploidy (30-39 chromosomes) are associated with unfavorable outcomes and require intensive treatment.4 The remaining patients, including TCF3-PBX1, are usually classified as intermediate risk, and those without an established chromosomal abnormality are referred to as B-other ALL.3
Recent genome-wide analysis has shown that mutations and, especially, copy-number alterations (CNAs) of genes involved in B-cell differentiation, cell cycle regulation, transcription, proliferation, and cell survival are common in BCP-ALL.5,6 The most frequently altered loci are EBF1, IKZF1, PAX5, CDKN2A/B, ETV6, BTG1, RB1, and PAR1 (for detection of P2RY8-CRLF2). The outcomes associated with these CNAs have been extensively studied, and prognostic markers have been described among them. For example, IKZF1 deletion, P2RY8-CRLF2 fusion, and PAX5 amplification have been linked to poor outcomes in some studies.7-14 However, there is evidence that the prognostic effect of secondary abnormalities is context dependent and can be modulated by the presence of other genetic abnormalities. For example, the prognostic effect of IKZF1 deletions appears worse when combined with BTG1 deletions or as a part of the newly described IKZF1plus profile.15,16 Notably, IKZF1 deletions do not adversely affect the good outcome associated with ERG deletions.17 Therefore, it is important to analyze the effect of different combinations of deletions and integrate them with other risk factors.
In our previous study, we used CNA data generated from consecutive childhood treatment trials, UKALL97/99 and UKALL2003, to define and validate a risk classifier (United Kingdom ALL [UKALL]–CNA).18 This classifier, which is based on the copy-number status of the 8 most commonly deleted regions in BCP-ALL, defined 3 CNA risk groups. Here, we further validate the classifier using a total 3239 patients collected from 12 clinical study groups who are all members of the International BFM (Berlin-Frankfurt-Munster) Study Group (iBFM). We confirm the robustness of this classifier and demonstrate how it interacts with cytogenetic and minimal residual disease (MRD) risk groups. Finally, we propose a revised integrated cytogenetic and CNA risk classification.
Methods
Patients
Patients eligible for this study were children and adolescents aged 1 to 19 years diagnosed with BCP-ALL before the end of 2014, treated on a clinical trial, and tested by multiplex ligation–dependent probe amplification (MLPA) using the SALSA P335 kit. All participating centers obtained local ethical committee approval and written informed consent in accordance with the Declaration of Helsinki. The demographic, clinical, genetic, and outcome data of the 3557 patients included were treated on 16 clinical trials collected from 12 study groups (supplemental Table 1). A total of 318 patients, who did not meet the inclusion criteria or had incomplete data, were excluded. Thus, 3239 patients, here after referred to as the iBFM cohort, were available for analysis. The number of patients, their recruitment period, follow-up time, and outcome varied among the study groups (supplemental Figure 1A-D).
Classification of cases
Genetic abnormalities were characterized by one or more of the following tests: cytogenetic analysis, fluorescence in situ hybridization, reverse transcription polymerase chain reaction, single-nucleotide polymorphisms, array or comparative genomic hybridization array. There was some variation in the distribution of cases by cytogenetic risk group (supplemental Figure 1E), which was driven by heterogeneous screening strategies. The high frequency of B-other ALL in Brazil, Poland, JACLS ALL-02, and Russia is likely due to the fact that not all cases were tested for all chromosomal abnormalities.
The copy-number status of EBF1, IKZF1, PAX5, CDKN2A/B, ETV6, BTG1, RB1, and PAR1 was determined using the SALSA MLPA kit P335 (MRC Holland, Amsterdam, The Netherlands) according to the manufacturer’s instructions. Each of these regions was coded, by the contributing study groups, as per the original study (see supplemental Methods)
We classified each patient in this cohort into 3 mutually exclusive risk groups based on the cytogenetic results (Figure 1A)3 and 3 mutually exclusive risk groups according to the UKALL-CNA classifier (Figure 1B),18 and we integrated the UKALL-CNA classifier with cytogenetic risk groups to generate a 2-tier genetic risk (Figure 1C).18
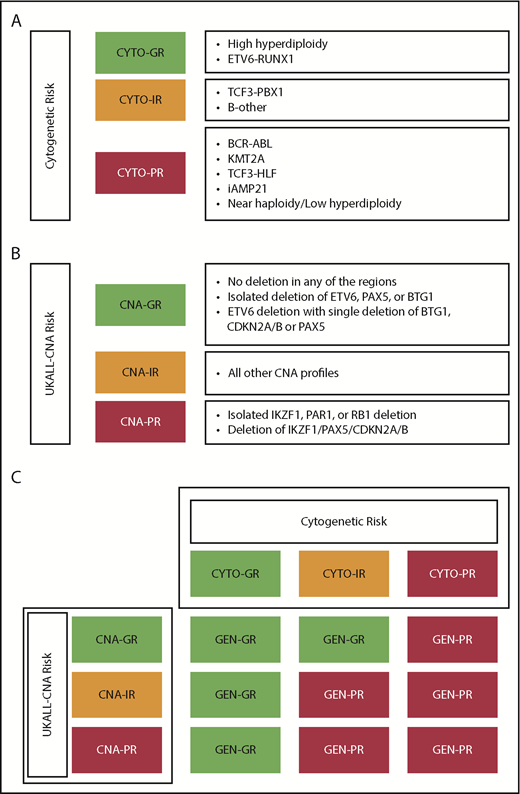
Definition of the cytogenetic, copy number alteration and integrated classifications used in this study. Definition of the classifiers used in the current study: cytogenetic (A), UKALL-CNA (B), and original genetic risk (C). CYTO, cytogenetic; GEN, genetics; GR, good risk; IR, intermediate risk; PR, poor risk.
Definition of the cytogenetic, copy number alteration and integrated classifications used in this study. Definition of the classifiers used in the current study: cytogenetic (A), UKALL-CNA (B), and original genetic risk (C). CYTO, cytogenetic; GEN, genetics; GR, good risk; IR, intermediate risk; PR, poor risk.
Statistical methods
As in the original study, we used event-free survival (EFS) as the primary end point, defining it as the time from the start of treatment to relapse, second tumor, or death, censoring at last contact and quoting 5-year rates. Secondary end points, relapse rate and overall survival, were considered but have not been presented, because there was no discordance between the rates. Only a small number of patients failed to achieve a complete remission (n = 51) or had a second tumor (n = 27). Survival rates were calculated and compared using Kaplan-Meier methods, log-rank tests, and univariate Cox regression models. Stratified Cox models were used to incorporate the effect of treatment risk group. Other comparisons were performed using χ2 or Fisher’s exact test as appropriate. Forest plots were drawn to depict the heterogeneity (ie, variation) in the effect between the study groups. Heterogeneity was tested using Higgins’s I2 measure of inconsistency.19 Statistically significant heterogeneity was defined as I2 ≥50% and a mild heterogeneity as between 25% and 50%. All tests were conducted at the 5% significance level. All analyses were performed using Intercooled Stata (StataCorp 2015 Stata Statistical Software Release 14; StataCorp, College Station, TX) and R version 3.4.3 (http://www.R-project.org).
Results
Direct validation of the UKALL-CNA classifier and genetic risk classification
Based on the copy-number status of the 8 defined loci, 106 unique CNA profiles were observed in the iBFM cohort. The most frequent CNA profile was “no deletions” and was observed in 40% of the cases. Among the remaining CNA profiles, 93 were observed in <1% of cases each, whereas only 5 profiles were present in ≥4% of cases. These 5 CNA profiles were the isolated deletion of CDKN2A/B (11%), ETV6 (7%), IKZF1 (4%), or PAX5 (4%) and the concurrent deletion of PAX5 and CDKN2A/B (5%) (supplemental Figure 2). There was a total of 29 new CNA profiles that had not been observed in the original UK study.18 However, these profiles were only observed in 45 cases and in total comprised <0.1% of cases. As per the original algorithm, cases with these profiles were assigned to the CNA-IR group.18
Overall, the majority of patients (58%) had a CNA-GR profile, with 33% and 9% of cases harboring a CNA-IR and CNA-PR profile, respectively (Figure 1B). The distribution of CNA risk groups varied between the study groups and was driven by the difference in frequency of regions specific alterations (supplemental Figure 1F). However, within each study group, the CNA-GR profile was the most prevalent (range, 50% to 72%), followed by CNA-IR (range, 22% to 40%) and finally CNA-PR (range, 5% to 10%) (supplemental Figure 1G). The UKALL-CNA classifier defined patients with distinct EFS (Figure 2A). Patients with a CNA-GR profile had a 50% reduced risk of an event compared with patients with a CNA-IR profile (Table 1), whereas patients with a CNA-PR profile had a 40% increased risk of an event compared with CNA-IR patients (Table 1). There was no evidence of heterogeneity across the 12 study groups for either comparison (both I2 = 0) (Figure 2B).
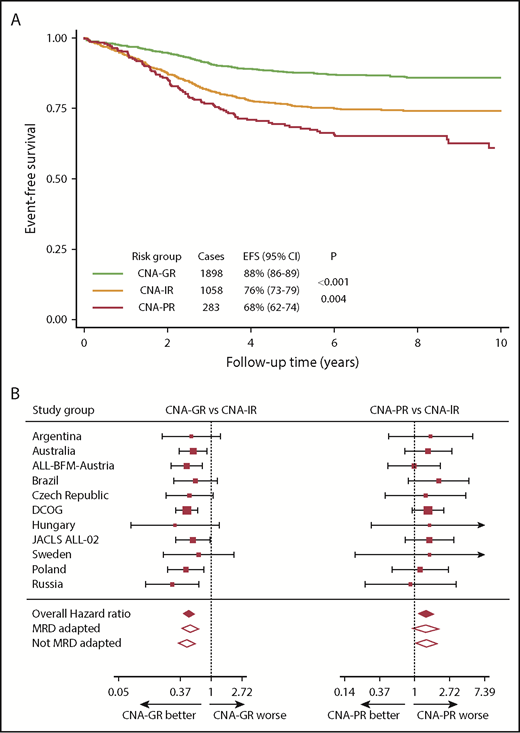
Outcome of 3239 patients in the iBFM cohort stratified by the UKALL-CNA classifier. (A-B) Kaplan-Meier survival curves (A) and forest plots depicting the hazard ratio and 95% CI from univariate Cox regression models comparing the EFS for CNA-GR or CNA-PR against CNA-IR (B). Patients in the Israeli National Study were excluded from the forest plot, as no event occurred in the CNA-GR or CNA-IR groups. DCOG, Dutch Childhood Oncology Group.
Outcome of 3239 patients in the iBFM cohort stratified by the UKALL-CNA classifier. (A-B) Kaplan-Meier survival curves (A) and forest plots depicting the hazard ratio and 95% CI from univariate Cox regression models comparing the EFS for CNA-GR or CNA-PR against CNA-IR (B). Patients in the Israeli National Study were excluded from the forest plot, as no event occurred in the CNA-GR or CNA-IR groups. DCOG, Dutch Childhood Oncology Group.
Cox regression models comparing the risk of an event between different genetic ungroups defined by the UKALL-CNA and revised genetic classifiers
| Classifier | Overall | MRD adapted | Non–MRD adapted | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hazard ratio | 95% CI | P | Hazard ratio | 95% CI | P | Hazard ratio | 95% CI | P | |
| Univariate models | |||||||||
| UKALL-CNA | |||||||||
| CNA-GR vs CNA-IR | 0.48 | 0.40-0.57 | <.001 | 0.51 | 0.39-0.66 | <.001 | 0.45 | 0.35-0.58 | <.001 |
| CNA-PR vs CNA-IR | 1.43 | 1.12-1.82 | .004 | 1.39 | 0.96-2.01 | .08 | 1.42 | 1.03-1.96 | .03 |
| Genetic risk | |||||||||
| GEN-GR vs GEN-VGR | 1.68 | 1.29-2.19 | <.001 | 1.33 | 0.93-1.91 | .12 | 2.19 | 1.46-3.29 | <.001 |
| GEN-IR vs GEN-GR | 2.05 | 1.65-2.53 | <.001 | 2.03 | 1.46-2.82 | <.001 | 2.03 | 1.53-2.69 | <.001 |
| GEN-PR vs GEN-IR | 1.95 | 1.51-2.53 | <.001 | 1.83 | 1.23-2.72 | .003 | 2.13 | 1.51-3.01 | <.001 |
| Models stratified by treatment risk group | |||||||||
| UKALL-CNA | |||||||||
| CNA-GR vs CNA-IR | 0.53 | 0.44-0.64 | <.001 | 0.53 | 0.41-0.70 | <.001 | 0.52 | 0.41-0.67 | <.001 |
| CNA-PR vs CNA-IR | 1.31 | 1.02-1.66 | .03 | 1.27 | 0.87-1.84 | .22 | 1.33 | 0.97-1.83 | .08 |
| Genetic risk | |||||||||
| GEN-GR vs GEN-VGR | 1.62 | 1.24-2.12 | <.001 | 1.30 | 0.90-1.89 | .16 | 2.06 | 1.37-3.09 | .001 |
| GEN-IR vs GEN-GR | 1.86 | 1.50-2.31 | <.001 | 1.89 | 1.36-2.65 | <.001 | 1.82 | 1.37-2.42 | <.001 |
| GEN-PR vs GEN-IR | 1.36 | 1.02-1.81 | .04 | 1.46 | 0.94-2.26 | .09 | 1.36 | 0.94-1.99 | .11 |
| Classifier | Overall | MRD adapted | Non–MRD adapted | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hazard ratio | 95% CI | P | Hazard ratio | 95% CI | P | Hazard ratio | 95% CI | P | |
| Univariate models | |||||||||
| UKALL-CNA | |||||||||
| CNA-GR vs CNA-IR | 0.48 | 0.40-0.57 | <.001 | 0.51 | 0.39-0.66 | <.001 | 0.45 | 0.35-0.58 | <.001 |
| CNA-PR vs CNA-IR | 1.43 | 1.12-1.82 | .004 | 1.39 | 0.96-2.01 | .08 | 1.42 | 1.03-1.96 | .03 |
| Genetic risk | |||||||||
| GEN-GR vs GEN-VGR | 1.68 | 1.29-2.19 | <.001 | 1.33 | 0.93-1.91 | .12 | 2.19 | 1.46-3.29 | <.001 |
| GEN-IR vs GEN-GR | 2.05 | 1.65-2.53 | <.001 | 2.03 | 1.46-2.82 | <.001 | 2.03 | 1.53-2.69 | <.001 |
| GEN-PR vs GEN-IR | 1.95 | 1.51-2.53 | <.001 | 1.83 | 1.23-2.72 | .003 | 2.13 | 1.51-3.01 | <.001 |
| Models stratified by treatment risk group | |||||||||
| UKALL-CNA | |||||||||
| CNA-GR vs CNA-IR | 0.53 | 0.44-0.64 | <.001 | 0.53 | 0.41-0.70 | <.001 | 0.52 | 0.41-0.67 | <.001 |
| CNA-PR vs CNA-IR | 1.31 | 1.02-1.66 | .03 | 1.27 | 0.87-1.84 | .22 | 1.33 | 0.97-1.83 | .08 |
| Genetic risk | |||||||||
| GEN-GR vs GEN-VGR | 1.62 | 1.24-2.12 | <.001 | 1.30 | 0.90-1.89 | .16 | 2.06 | 1.37-3.09 | .001 |
| GEN-IR vs GEN-GR | 1.86 | 1.50-2.31 | <.001 | 1.89 | 1.36-2.65 | <.001 | 1.82 | 1.37-2.42 | <.001 |
| GEN-PR vs GEN-IR | 1.36 | 1.02-1.81 | .04 | 1.46 | 0.94-2.26 | .09 | 1.36 | 0.94-1.99 | .11 |
CI, confidence interval; VGR, very good risk.
MRD is also an important risk factor in pediatric ALL, and studies have demonstrated the benefit of using MRD to determine treatment intensity.20-22 Moreover, the prognostic effect of other CNA and gene expression profiles, IKZF1plus and BCR-ABL1-like, have been shown to be modulated by MRD.23,24 Therefore, we reexamined the prognostic effect of the UKALL-CNA classifier stratifying by protocol type (ie, whether or not treatment was altered on the basis of MRD; MRD adapted vs non–MRD adapted) (supplemental Table 1). Even among the 1753 patients treated on MRD-adapted protocols, the UKALL-CNA classifier defined subgroups that were prognostic (supplemental Figure 3A). However, the difference between CNA-IR and CNA-PR was not significant (P = .08). As expected the UKALL-CNA classifier was highly prognostic among the remaining 1486 patients treated on protocols that did not alter treatment on the basis of MRD (supplemental Figure 3B). The hazard ratios for CNA-GR vs CNA-IR and CNA-PR vs CNA-IR did not differ according to the type of protocol (ie, MRD adapted or not) (Table 1; Figure 2B). In addition, there was no evidence of heterogeneity between different MRD-adapted protocols or between the remaining protocols (I2 = 0%) (Figure 2B). Furthermore, stratifying by treatment risk group did not materially alter the hazard ratios comparing the different subgroups (Table 1).
In our previous study,18 we integrated the newly defined CNA subgroups with classical cytogenetic risk groups (Figure 1C) to derive 2 genetic risk groups: GEN-GR and GEN-PR. Replicating this definition on the iBFM cohort produced 2 subgroups comprising 71% and 29% cases, respectively. For most study groups, the distribution of genetic risk groups was similar, except for Brazil, the Israeli National study, and JACLS ALL-02 (supplemental Figure 1). This variation was driven by incomplete screening strategies. Within this cohort, GEN-GR patients had a significantly higher EFS rate than GEN-PR patients (88% [86-89] vs 69% [66-72], P < .001) (Figure 3A). GEN-PR patients were almost 3 times more likely to suffer an event compared with GEN-GR patients (hazard ratio, 2.92; 95% CI, 2.46-3.47; P < .001). There was no evidence of heterogeneity across the 12 study groups (I2 = 0). However, mild heterogeneity in the hazard ratios was found between MRD-adapted and non–MRD-adapted trials (I2 = 40%) (Figure 3B).
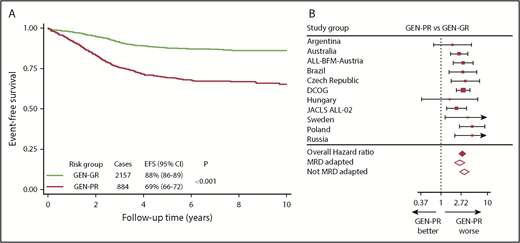
Outcome of 3239 patients in the iBFM cohort stratified by the original genetic risk group. (A-B) Kaplan-Meier survival curves (A) and forest plot (B) depicting the hazard ratio and 95% confidence interval from univariate Cox regression models comparing the EFS for GEN-PR vs GEN-GR. Patients in the Israeli National Study were excluded from the forest plot, as no event occurred in the GEN-GR group.
Outcome of 3239 patients in the iBFM cohort stratified by the original genetic risk group. (A-B) Kaplan-Meier survival curves (A) and forest plot (B) depicting the hazard ratio and 95% confidence interval from univariate Cox regression models comparing the EFS for GEN-PR vs GEN-GR. Patients in the Israeli National Study were excluded from the forest plot, as no event occurred in the GEN-GR group.
Prognostic effect of the UKALL-CNA classifier within cytogenetic risk groups
We classified all patients in the iBFM cohort according to the UK-defined cytogenetic risk groups.3 Overall, the 3 risk groups comprised 48% (CYTO-GR), 46% (CYTO-IR), and 6% (CYTO–high risk [HR]) of patients. The distribution of these risk groups varied across the 12 study groups (supplemental Figure 1E), reflecting the different definition of cytogenetic risk used by the study groups according to their screening strategies. The majority of CYTO-GR patients had a CNA-GR profile (69%), while the remaining patients were assigned to either CNA-IR (26%) or CNA-PR (5%). In contrast, 50% CYTO-IR patients had a CNA-GR profile, while patients in the remaining half were either CNA-IR (39%) or CNA-PR (11%). Only 44% of CYTO-HR patients had a CNA-GR profile, while 38% and 18% of the patients had CNA-IR and CNA-PR profiles, respectively (supplemental Figure 4).
Within the CYTO-GR group, the 3 CNA risk groups were associated with significantly different EFS rates of 91% (89-93) vs 85% (81-89) vs 73% (60-82) (P < .001) for CNA-GR vs CNA-IR vs CNA-PR, respectively (Figure 4A). CYTO-GR/CNA-GR patients had a 42% reduced risk of an event compared with those with the CYTO-GR/CNA-IR (hazard ratio, 0.58; 95% CI, 0.42-0.81; P = .002). The CYTO-GR/CNA-PR patients had an 85% increased risk of an event compared with CYTO-GR/CNA-IR patients (hazard ratio, 1.85; 95% CI, 1.10-3.11; P = .02. Further subgroup analysis revealed the same effect when ETV6-RUNX1 and high hyperdiploidy patients were considered separately (supplemental Figure 5). There was no evidence of heterogeneity across the 12 study groups for either the positive effect of CNA-GR or the negative effect of CNA-PR within CYTO-GR patients (both I2 = 0). However, when we analyzed these effects by protocol type (MRD and non–MRD driven), we did observe significant (I2 = 72%) and mild (I2 = 45%) heterogeneity, respectively (supplemental Table 2). The beneficial effect of a CNA-GR profile was restricted to those CYTO-GR patients treated on protocols that did not change therapy on the basis of MRD. In contrast, the adverse effect of a CNA-PR profile appeared to be limited to patients treated on MRD-adapted protocols.
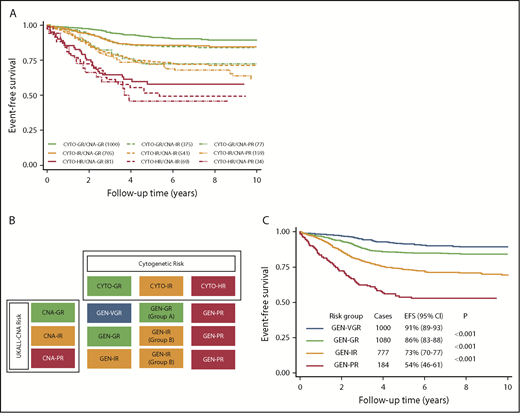
Integration of cytogenetic and CNA subgroups using the 3239 patients in the iBFM cohort reveals a new genetic risk classification. (A) EFS of the 9 subgroups derived from cross-tabulating the 3 cytogenetic and 3 CNA risk groups. (B) Visualized inspection of these curves reveals 4 overall genetic risk groups. (C) EFS of the revised genetic risk groups, which are significantly different from one another.
Integration of cytogenetic and CNA subgroups using the 3239 patients in the iBFM cohort reveals a new genetic risk classification. (A) EFS of the 9 subgroups derived from cross-tabulating the 3 cytogenetic and 3 CNA risk groups. (B) Visualized inspection of these curves reveals 4 overall genetic risk groups. (C) EFS of the revised genetic risk groups, which are significantly different from one another.
Among CYTO-IR patients, the EFS rates across the 3 CNA risk groups was 86% (83-88), 74% (70-78), and 72% (64-79) for CNA-GR, CNA-IR, and CNA-PR, respectively (Figure 4A). There was no statistically significant difference between CYTO-IR/CNA-IR and CYTO-IR/CNA-PR (P = .28). In our previous study, we combined CYTO-IR/CNA-IR and CYTO-IR/CNA-PR patients (group B) and compared their outcome to CYTO-IR/CNA-GR (group A).18 Replicating this analysis in the iBFM cohort revealed that group B patients had a significantly inferior EFS at 5 years (P < .001, Figure 5A) and were twice as likely to have an adverse event as group A patients (hazard ratio, 2.09; 95% CI, 1.62-2.69; P < .001). No evidence of heterogeneity was observed across the 12 study groups or across the 2 main protocol types (MRD adapted and non–MRD adapted) (Figure 5B).
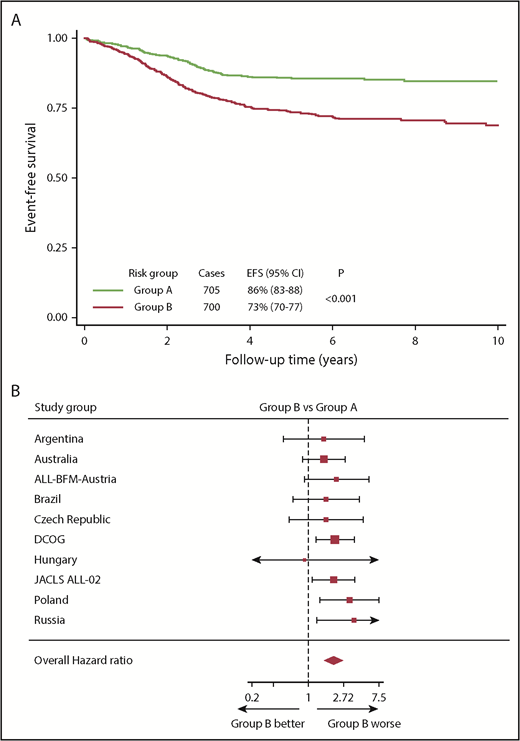
Outcome of 1405 patients in the iBFM cohort with IR cytogenetics classified according to their CNA profile. (A-B) Kaplan-Meier survival curves (A) and forest plot (B) depicting the hazard ratio and 95% confidence interval from univariate Cox regression models comparing the EFS for group B (CYTO-IR/CNA-IR and CYTO-IR/CNA-PR) vs group A (CYTO-IR/CNA-GR). Patients in the Israeli National and Sweden studies were excluded from the forest plot, as no event occurred in group B.
Outcome of 1405 patients in the iBFM cohort with IR cytogenetics classified according to their CNA profile. (A-B) Kaplan-Meier survival curves (A) and forest plot (B) depicting the hazard ratio and 95% confidence interval from univariate Cox regression models comparing the EFS for group B (CYTO-IR/CNA-IR and CYTO-IR/CNA-PR) vs group A (CYTO-IR/CNA-GR). Patients in the Israeli National and Sweden studies were excluded from the forest plot, as no event occurred in group B.
There was no evidence of outcome heterogeneity by CNA profile among patients with HR cytogenetics (ie, CYTO-HR) (58% [46-68] vs 52% [38-63] vs 46% [27-63], P = .55, CNA-GR vs CNA-IR vs CNA-PR, respectively) (Figure 4A).
A revised genetic risk classification for BCP-ALL
Visual inspection of the EFS curves of the 9 subgroups, which resulted from integrating the UKALL-CNA and cytogenetic subgroups (Figure 4A), revealed the presence of 4 discrete genetic risk groups: GEN-VGR, GEN-GR, GEN-IR, and GEN-PR (Figure 4B). These groups comprised 33%, 36%, 26% and 6% cases, respectively, and had significantly different outcomes (Figure 4C). Patients in the GEN-VGR group, which comprised patients with both GR cytogenetics and GR CNA features, had an excellent EFS rate, which was significantly better than the EFS of the remaining patients in the CYTO-GR group and the patients in the CYTO-IR/CNA-IR group (GEN-GR). Thus, patients in the revised GEN-GR group had a 68% higher risk of an event compared with those patients in GEN-VGR group (Table 1). In contrast, patients categorized in the GEN-IR group (composed mainly of CYTO-IR patients who have a CNA-GR/IR profiles [91%] and CYTO-GR patients who have CNA-PR profiles [9%]) had an EFS rate of 73% (70% to 77%). This meant that GEN-IR patients were twice as likely to suffer an event compared with GEN-GR patients (Table 1). Patients in the GEN-PR group, comprised solely of those patients with HR cytogenetics, were almost twice as likely to have an event than GEN-IR patients (Table 1). Overall, there was little evidence for heterogeneity across the participating study groups (supplemental Table 4). However, there was mild heterogeneity for the GEN-PR vs GEN-IR comparison (I2 = 37%), but this was likely driven by small numbers. When we assessed heterogeneity by protocol type (MRD adapted or non–MRD adapted), we noted that the difference between the GEN-VGR and GEN-GR groups was only seen for patients treated on protocols that were non–MRD adapted (Table 1). This revised genetic classification was validated in the original UK trial datasets (supplemental Figure 6; supplemental Table 3). Consistent with the heterogeneity observed in the iBFM cohort, there was no difference between the GEN-VGR and GEN-GR subgroups in UKALL2003 (supplemental Figure 6B), which used MRD to adapt therapy, compared with UKALL97/99 (supplemental Figure 6A), which did not use MRD. Overall, adjusting for the effect of treatment did not alter the prognostic impact of the revised genetic classification (Table 1).
Discussion
The primary objective of this validation study was to assess whether our previously defined UKALL-CNA classifier18 was prognostic in non-UK treatment protocols. The results of our analysis clearly demonstrated that the UKALL-CNA profile was indeed prognostic across a range of treatment protocols used by 12 different study groups (supplemental Figure 1). The hazard ratios, which measure the relative risk of an event among the 3 CNA risk groups, derived from the iBFM cohort were remarkably similar to those derived from the 2 original cohorts. The hazard ratios for CNA-GR vs CNA-IR in ALL97 and UKALL2003 were 0.48 (95% CI, 0.40-0.57; P < .001) and 0.50 (95% CI, 0.40-0.64; P < .001), respectively. In addition, the hazard ratios for CNA-PR vs CNA-IR were 1.43 (95% CI, 1.12-1.82; P = .004) and 1.44 (95% CI, 1.04-1.99; P = .03), respectively. Moreover, we demonstrated that the UKALL-CNA classifier provides relevant prognostic information within both MRD-adapted and non–MRD-adapted protocols (supplemental Figure 3). Pediatric ALL protocols do not vary greatly in the core chemotherapeutic drugs used or in the proportion of patients that receive a stem cell transplant. However, they do differ in terms of risk stratification, drug dosing, and scheduling. The study groups involved in this meta-analysis span a wide range of countries across 4 continents and 18-year treatment period. Despite this extensive variation, the prognostic relevance of the UKALL-CNA classifier was consistent across different protocols and treatment risk groups (Table 1). Therefore, we conclude that the UKALL-CNA classifier is a robust tool for defining prognostic risk groups in pediatric BCP-ALL.
In addition to validating the UKALL-CNA classifier as a standalone tool, we also investigated how it integrated with our published cytogenetic risk groups.3 In our previous study, we showed that the UKALL-CNA classifier did not add prognostic information to the CYTO-GR or CYTO-HR groups. The results of this much larger meta-analysis confirmed that patients in the CYTO-HR group had a poor outcome irrespective of CNAs. However, in contrast to the original study, we found significant outcome heterogeneity by CNA profile among CYTO-GR patients (supplemental Table 2). The explanations for such a difference include treatment period, screening strategies, and patient numbers. However, given that the differences between CNA-GR and CNA-IR were confined to non–MRD-adapted protocols, which were generally from earlier time periods, it suggested that the difference might have been caused by the iBFM cohort spanning a longer treatment period compared with the original study (>20 vs <15 years). We also observed a significantly inferior outcome for CYTO-GR/CNA-PR patients compared with CYTO-GR/CNA-IR patients (supplemental Table 2). Interestingly, this prognostic effect was stronger among patients treated on MRD-adapted protocols, supporting the notion that integrating MRD and genetics improves risk prediction.24
We also validated the prognostic utility of the 2-tier genetic classification proposed in the UK study18 (Figure 3). The large number of patients collected enabled us to integrate cytogenetics with the UKALL-CNA classifier in more depth, which defined 4 genetic risk groups (Figure 4). The original GEN-GR group could be split into VGR, GR, and IR groups, while the original GEN-PR group can be divided into an IR and PR groups. There was little heterogeneity across these revised risk groups by study group (supplemental Table 4). The mild heterogeneity observed for the GEN-PR vs GEN-IR comparison could be explained by the incomplete screening for HR cytogenetic abnormalities in some study groups and also by treatment differences, which are more pronounced for HR patients. There was significant heterogeneity comparing the outcome of GEN-VGR vs GEN-GR patients by protocol type, such that the improved outcome for GEN-VGR patients was not observed in MRD-adapted protocols, including UKALL2003 (supplemental Figure 6). This finding is consistent with our observation that within the CYTO-GR group, only CNA-GR patients treated on a non–MRD-adapted protocol have a superior outcome to CYTO-GR/CNA-IR patients (supplemental Table 2).
Our study has a number of strengths but also some limitations. The major strengths are the number of cases collected and breadth of contributing studies, including protocols that used MRD to adapt treatment intensity. These 2 factors enabled us to validate the UKALL-CNA classifier across a heterogeneous collection of protocols to confirm that its prognostic impact is robust. However, as we collected data from so many study groups, we were not able to collect and analyze the raw MLPA data. It is conceivable that there was variation in the calling of deletions between countries. Although there was variation in the frequency of deletions across the 12 study groups (supplemental Figure 1) as well as between the iBFM cohort and the original discovery cohort (supplemental Table 3), it was not large, and there was no evidence of systematic miscalling. Each study group followed the manufacturer’s guidelines, called deletions according to the definition in the original study, and mostly had experience of >100 MLPA tests. Discussions with the contributing authors revealed only one significant area of variation between groups, which was the calling of single probe loss. In line with our original study, we did not consider single probe loss as a deletion. However, this is an important question that must be addressed when prospectively calling the CNA profile in future studies. The main limitation of this meta-analysis was the reliance on cytogenetic data derived from different testing strategies. Screening for key prognostic chromosomal abnormalities, particularly those associated with HR disease (eg, iAMP21), was not systemically performed across study groups, which is in contrast to the original UK study. Importantly, this did not affect the primary objective of validating the UKALL-CNA classifier. We were careful to only include patients in the B-other/CYTO-IR subgroups who had tested negative for the most prevalent chromosomal abnormalities, so the number of misclassified cases is likely to be small. We recognize that exclusion of cases that had not been fully tested generated relatively large B-other subgroups. However, because none of our analyses were sensitive to the relative size of the 3 cytogenetic risk groups, this did not impact the validity of our results. Although we did not have individual patient MRD data, we validated the classifiers by examining their effect in MRD adapted and non-adapted trials separately as well as by stratifying by treatment risk group. Both the UKALL-CNA and genetic classifiers were remarkably stable highlighting the added benefit in MRD driven protocols. The reduction in hazard ratio observed when we compared GEN-PR and GEN-IR patients adjusting for treatment (Table 1) is likely to be driven by HR patients receiving specific interventions (eg, transplant).
The validation of the UKALL-CNA classifier confirms its widespread clinical utility. Even though it is based on the 8 most prevalent CNAs, it is conceivable that additional CNAs or profiles could define additional information. Indeed the German and Italian study groups have recently published a CNA profile termed IKZF1plus.16 Patients are classified as IKZF1plus if they harbor an IKZF1 deletion plus a deletion involving CDKN2A/B, PAX5, or PAR1, unless they have a concurrent ERG deletion. The frequency of IKZF1plus is ∼6% among BCP-ALL patients, and it is associated with a poor outcome in MRD-positive patients. Both profiles highlight the prognostic importance of CNA in predicting outcome in pediatric ALL. Moreover, there is a great deal of similarity between the definition of IKZF1plus and the profiles classified into the UKALL-CNA-PR group. While IKZF1plus defines a small group of PR patients and is MRD dependent, the UKALL-CNA classifier applies to all patients and defines 3 risk groups that are prognostic even in MRD-adapted protocols. One of the major advantages of the UKALL-CNA classifier is the ability to subdivide the CYTO-IR cohort into subgroups with significantly different outcomes (Figure 5). Importantly, and confirming the findings of our original study, CYTO-IR/CNA-GR patients have an outcome very similar to that of CYTO-GR patients. We have recently shown that patients with both GR genetics and rapid disease clearance have a very low risk of relapse.8,24 These observations raise the possibility of defining a very large subset of patients, which could be considered for treatment deescalation to avoid future long-term toxicity.
In conclusion, we have validated the prognostic impact of the UKALL-CNA classifier using a cohort of 3239 patients treated on 16 trials including MRD-adapted protocols. This study adds to the body of evidence that supports the prognostic effect of secondary abnormalities in ALL. The integration of CNA and cytogenetic risk group proves the context-dependent nature of this effect and enables the definition of clinically relevant genetic risk groups. We propose that these data support the use of the UKALL-CNA classifier in future risk-stratification algorithms.
The full-text version of this article contains a data supplement.
Acknowledgments
The authors thank the following people for assistance in producing and collating data: Caroline Barbieri, Thayana C. Barbosa, Pauline Dalzell, Jorge A. Digiorge, Alexander Druy, Eugenia T. Granado, Glenn Marshall, Tallita Meciany, and Anthea Ng.
This study was supported by Bloodwise (A.V.M. and C.J.H.), the Bloodwise Childhood Cell Bank (A.V.M. and C.J.H.), the Anniversary Fund of the Oesterreichische Nationalbank (OeNB 14133) (K.N.), Brazilian National Council for Scientific and Technological Development (CNPq) (PQ-2017#305529/2017-0) and Fundacao Carlos Chagas Filho de Amparo a Pesquisa do Estado do Rio de Janeiro (E_26/201.539/2014 and E_26/203.214/2017) (M.E.), Polish Ministry of Science and Higher Education “Diamond Grant” (DI2012017042) (M.B.), National Center of Research and Development (NCBiR project LIDER 031/635/l-5/13/NCBR/2014) (A.P.) (NCBiR project STRATEGMED3/304586/5/2017 PersonALL (W.M.), Grants for Clinical Cancer Research from the Ministry of Health, Labour and Welfare of Japan (H14-Koka (Gan)-031, H15-Koka (Gan)-024, H16-GanRinsho-004, H17-GanRinsho-004), Ministry of Health of the Czech Republic (grant 16-32568A) and Ministry of Education, Youth and Sports of the Czech Republic (NPU I LO1604) (E.F. and J.T.), the Israel Cancer Association (S.E. and M.J.), the Netherlands Organisation for Scientific Research, the Dutch Cancer Society, the Kika Foundation and the Pediatric Oncology Foundation Rotterdam, the National Health and Medical Research Council Australia and Cancer Council NSW (R.S. and L.D.P.), and CNPq#301594/2015-5 (M.S.P.-d.-O.)
Authorship
Contribution: A.V.M. and A.E. conceived and designed the study; L.H., A.E., C.S., G.B., M.L.d.B., J.M.B., M.B., S.E., M.E., L.F., M.S.F., E.F., K.H., T.I., M.J., R.P.K., W.M., K.N., I.I.Ö., I.H.,H.P., P.R., S.S., R.S., J.T., G.T., N.V., M.Y., A.V., and A.V.M collected and assembled the data; L.H., A.E., and A.V.M. analyzed and interpreted the data; C.J.H. and A.V.M. provided financial and administrative support; C.N.A., A.A., L.D.P., M.M.H., I.H., G.K., A.P., R.P., M.S.P.-d.-O., J.S., and A.V. provisioned the study materials and patients; L.H., A.V.M., and A.E. wrote the manuscript; and all authors approved the final manuscript.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
A complete list of the members of the International BFM Study Group appears in the supplemental appendix.
Correspondence: Anthony V. Moorman, Leukaemia Research Cytogenetics Group, Wolfson Childhood Cancer Research Centre, Northern Institute for Cancer Research, Newcastle University, Level 6, Herschel Building, Brewery Ln, Newcastle upon Tyne NE1 7RU, United Kingdom; e-mail: anthony.moorman@newcastle.ac.uk.

