

Background: Measurable residual disease (MRD) by multiparameter flow cytometry (MFC) is highly prognostic for relapse and overall survival (OS) in patients (pts) with acute lymphoblastic leukemia (ALL). However, many pts with apparent "MRD negativity" by MFC still relapse. These relapses are likely due to residual leukemia that is present below the level of detection of MFC (generally ~1x10-4). In light of the limitations of conventional MRD assays, we sought to evaluate the clinical impact of a highly sensitive next-generation sequencing (NGS)-based MRD assay that is capable of detecting residual leukemia at a level of 1x10-6.
Methods: We performed a retrospective study of 67 pts with previously untreated Philadelphia chromosome-negative ALL who received frontline therapy between 2/2012 and 7/2018 with a hyper-CVAD-based regimen (n=44) or a lower-intensity hyper-CVD-based regimen (n=23), which was usually combined with inotuzumab ozogamicin, and achieved complete remission (CR). Pts were selected for this study based on availability of banked samples at baseline and at sequential remission time points up to 4.5 months after start of therapy. Six-color MFC was performed as standard of care with an analytic sensitivity of 0.01% (1x10-4). Pretreatment genomic DNA derived from bone marrow was evaluated using a quantitative NGS MRD assay (Adaptive Biotechnologies Co., Seattle, WA) to identify dominant rearrangements within the B-cell receptor (IgH [VDJ and DJ], IgK and IgL). High throughput NGS of remission samples was subsequently performed to assess the target clonal rearrangements at an established analytic sensitivity of 0.0001% (1x10-6).
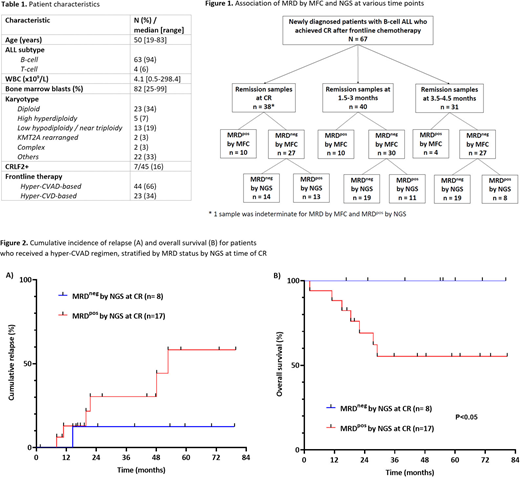
Results: The baseline characteristics of the study population are shown in Table 1. Twenty pts (30%) underwent allogeneic stem cell transplant (alloSCT) in first remission. In the entire cohort, 14 pts relapsed (21%), including 2 with CNS-only relapses. The median duration of follow-up for the entire cohort was 51 months.
Among the 109 remission samples, 84 were MRD-negative (MRDneg), 24 were MRD-positive (MRDpos), and 1 was indeterminate by MFC (Figure 1). All 24 MRDpos samples by MFC were also MRDpos by NGS. Among the 84 MRDneg samples by MFC, 32 (38%) were MRDpos by NGS. For these discordant cases, the median level of MRD by NGS was below the expected level of detection by MFC (median 0.002% [range 0.00002%-1.15%]).
At the time of CR, 44/67 pts (66%), achieved MRDneg by MFC and 14/38 (37%) achieved MRDneg by NGS. The rates of MRDneg by MFC in pts treated with hyper-CVAD or hyper-CVD regimens were 61% and 74%, respectively, and by NGS were 32% and 46%, respectively. Achieving MRDneg by NGS at the time of CR better predicted the likelihood of durable remission than did achieving MRDneg by MFC. The 5-year cumulative incidence of relapse (CIR) of the 44 pts who achieved MRDneg by MFC and of 14 pts who achieved MRDneg by NGS was 27% and 8%, respectively. Only 1 out of 14 pts who achieved MRDneg by NGS at the time of CR subsequently relapsed. In contrast, MRD status by NGS did not predict for relapse when evaluated at post-CR time points.
Among pts treated with a more intensive hyper-CVAD regimen, achievement of MRDneg by NGS at CR provided additional prognostic information compared to MRD status by MFC at the same time point and identified pts with an excellent long-term outcome. The 5-year OS rate for pts who achieved MRDneg by NGS at CR was 100% vs. 55% for those who were MRDpos by NGS (Figure 2A; P<0.05). This superior outcome was driven by the lower CIR rate in the MRDneg pts (Figure 2B; 5-year CIR: 13% vs. 58% in MRDpos pts). The impact of achieving MRDneg by NGS at CR was particularly evident in pts who did not undergo alloSCT in first remission where the 5-year CIR rates were 14% and 81%, respectively. When integrating MRD information by MFC and NGS, the 5-year OS rate for pts who were MRDneg by both MFC and NGS, MRDneg by MFC but MRDpos by NGS, and MRDpos by both MFC and NGS were 100%, 67%, and 38%, respectively (P=0.02 for trend). Similarly, the 5-year CIR rates were 13%, 57%, and 63%, respectively.
Conclusion: Early assessment of MRD using an ultrasensitive NGS assay can identify pts with ALL who have a very low risk of relapse and excellent long-term survival. Prospective studies are warranted to assess whether de-intensification of therapy is feasible for this favorable-risk group of pts who rapidly achieve MRDneg remission.
Short:Amgen: Honoraria; Astellas: Research Funding; AstraZeneca: Consultancy; Takeda Oncology: Consultancy, Honoraria, Research Funding. Kantarjian:Takeda: Honoraria; Amgen: Honoraria, Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Cyclacel: Research Funding; Pfizer: Honoraria, Research Funding; Agios: Honoraria, Research Funding; Novartis: Research Funding; Immunogen: Research Funding; AbbVie: Honoraria, Research Funding; BMS: Research Funding; Ariad: Research Funding; Jazz Pharma: Research Funding; Daiichi-Sankyo: Research Funding; Astex: Research Funding. Konopleva:F. Hoffmann La-Roche: Consultancy, Research Funding; Eli Lilly: Research Funding; Cellectis: Research Funding; Calithera: Research Funding; Rafael Pharmaceutical: Research Funding; Amgen: Consultancy; Sanofi: Research Funding; Stemline Therapeutics: Consultancy, Research Funding; Ablynx: Research Funding; Agios: Research Funding; AbbVie: Consultancy, Research Funding; Ascentage: Research Funding; AstraZeneca: Research Funding; Forty-Seven: Consultancy, Research Funding; Reata Pharmaceutical Inc.;: Patents & Royalties: patents and royalties with patent US 7,795,305 B2 on CDDO-compounds and combination therapies, licensed to Reata Pharmaceutical; Kisoji: Consultancy; Genentech: Consultancy, Research Funding. Jain:Cellectis: Research Funding; BMS: Research Funding; BeiGene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Verastem: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Fate Therapeutics: Research Funding; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Research Funding; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Aprea Therapeutics: Research Funding; Pharmacyclics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Incyte: Research Funding; Genentech: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; ADC Therapeutics: Research Funding; TG Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees; Precision Bioscienes: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Adaptive Biotechnologies: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AstraZeneca: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Kebriaei:Kite: Other: Served on advisory board; Amgen: Other: Research Support; Ziopharm: Other: Research Support; Pfizer: Other: Served on advisory board; Novartis: Other: Served on advisory board; Jazz: Consultancy. Yilmaz:Pfizer: Research Funding; Daicho Sankyo: Research Funding; Pint Pharma: Honoraria. Issa:Celegene: Research Funding; Syndax: Research Funding; Novartis: Membership on an entity's Board of Directors or advisory committees. Ravandi:BMS: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; Astellas: Consultancy, Honoraria, Research Funding; Xencor: Consultancy, Honoraria, Research Funding; Macrogenics: Research Funding; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Orsenix: Consultancy, Honoraria, Research Funding. Jabbour:Amgen: Other: Advisory role, Research Funding; Adaptive Biotechnologies: Other: Advisory role, Research Funding; BMS: Other: Advisory role, Research Funding; Genentech: Other: Advisory role, Research Funding; AbbVie: Other: Advisory role, Research Funding; Takeda: Other: Advisory role, Research Funding; Pfizer: Other: Advisory role, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal