

TO THE EDITOR:
Advanced age is a risk factor for large B-cell lymphomas and is associated with an increased risk of relapse and death.1,2 Relapses in patients with chemotherapy-sensitive disease may be treated with high-dose chemotherapy, followed by autologous stem-cell transplantation (ASCT).3 However, outcomes are historically poor among patients who require salvage therapy,4 and although the feasibility of aggressive therapies in older patients has been demonstrated,5 physicians may be reluctant to administer them because of concerns about toxicity or comorbidities.6 Thus, the inclusion of older patients is important in trials evaluating new therapies for relapsed or refractory large B-cell lymphomas.
Axicabtagene ciloleucel (axi-cel), an autologous anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, is approved in multiple countries for the treatment of patients with relapsed or refractory large B-cell lymphoma after failure of 2 or more systemic therapies.7,8 Regulatory approvals were based on the results of the ZUMA-1 study, which evaluated axi-cel in relapsed or refractory large B-cell lymphoma.9,10 In a 2-year analysis of ZUMA-1, by investigator assessment, axi-cel demonstrated objective, complete, and ongoing response rates of 83%, 58%, and 39%, respectively.9 Here, we report additional 2-year results from ZUMA-1, a post hoc subgroup analysis of efficacy and safety in patients ≥65 vs those <65 years of age.
Details of the ZUMA-1 study design have been reported.9-11 In brief, this was a single-arm, phase 1/2 study in adults with refractory diffuse large B-cell lymphoma (DLBCL), primary mediastinal B-cell lymphoma, or transformed follicular lymphoma. Refractory disease was defined as no response to last chemotherapy, or relapse ≤12 months after ASCT. Patients were also required to have an Eastern Cooperative Oncology Group performance status of 0 or 1 and to have received prior treatment with both an anti-CD20 monoclonal antibody and an anthracycline-containing regimen. After a conditioning regimen of cyclophosphamide (500 mg/m2 per day) and fludarabine (30 mg/m2 per day) for 3 days, patients received 1 dose of axi-cel (2 × 106 CAR T cells per kg). The cutoff date for the current analysis was 11 August 2018, and patients were followed up for a minimum of 24 months from the axi-cel infusion (median follow-up was 27.1 months). Safety assessments included all treated patients enrolled in phases 1 and 2 (≥65 y, n = 27; <65 y, n = 81). Efficacy assessments included treated patients in phase 2 only (≥65 y, n = 24; <65 y, n = 77). All authors participated in the development of the analysis plan and had full access to all analysis results. Each study site’s institutional review board reviewed and approved the study protocol and amendments, and all patients provided written informed consent. This trial was registered at clinicaltrials.gov as #NCT02348216.
Baseline characteristics were largely similar between patients ≥65 years of age and patients <65 years of age, with some exceptions (Table 1). Most notably, a numerically greater proportion of patients in the ≥65 age group than in the <65 age group had an International Prognostic Index (IPI) score of 3 to 4, which is attributable to age >60 years being a component of IPI scoring.2 A greater proportion of patients <65 years had received ASCT, as those ≥65 years were less likely to be considered for ASCT. CAR T-cell expansion in vivo was similar for patients ≥65 and those <65 years of age (median peak expansion, 43.0 and 35.3 CAR T cells per µL blood, respectively; P = .769; median area under the curve, 562.0 and 448.4 CAR T cells per µL, respectively, from days 0 to 28; P = .983). Efficacy outcomes are summarized in Table 1 and Figure 1A-B. Investigator-assessed objective response rates (ORRs) were comparable: 92% for patients ≥65 and 81% for patients <65 years of age. A numerically greater proportion of patients aged ≥65 years than of those aged <65 years had complete response as the best response (75% vs 53%, respectively) and ongoing response at data cutoff (42% vs 38%, respectively). A similar trend was observed when response rates were assessed by histological subtypes (supplemental Table 1; available on the Blood Web site). Median duration of response (DOR) was 12.0 months for patients ≥65 and 8.1 months for those <65 years of age. Median progression-free survival (PFS) was 13.2 months for patients ≥65 years of age and 5.6 months for those <65 years of age. Approximately 50% of patients in both age groups were alive at 24 months after treatment (≥65 years, 54%; <65 years, 49%). Efficacy outcomes in ZUMA-1 compare favorably with those reported in the 2017 SCHOLAR-1 study,4 a pooled, retrospective analysis of 636 patients with DLBCL that was resistant to chemotherapy or who relapsed within 12 months of ASCT. In patients ≥65 and <65 years of age, available therapies in the pre-CAR T-cell era resulted in ORRs of only 19% and 27%, respectively, and 2-year survival rates of 19% and 20%, respectively.4
Patient characteristics, efficacy, and safety
| Characteristic | ≥65 y (n = 27) | <65 y (n = 81) |
|---|---|---|
| Median age (range), y | 69 (65-76) | 55 (23-64) |
| Male, n (%) | 22 (81) | 51 (63) |
| ECOG performance status 1, n (%) | 16 (59) | 46 (57) |
| Disease stage III/IV, n (%) | 22 (81) | 68 (84) |
| IPI score 3-4, n (%) | 19 (70) | 29 (36) |
| ≥3 Prior therapies, n (%) | 18 (67) | 58 (72) |
| Median tumor burden by SPD (range), mm2 | 3 790 (600-16 764) | 3 574 (171-23 297) |
| Disease type, n (%) | ||
| DLBCL | 20 (74) | 64 (79) |
| PMBCL | 0 | 8 (10) |
| TFL | 7 (26) | 9 (11) |
| Prior ASCT, n (%) | 5 (19) | 24 (30) |
| Refractory subgroup before enrollment, n (%) | ||
| Primary refractory | 1 (4) | 2 (2) |
| Refractory to second-lineor later therapy | 21 (78) | 59 (73) |
| Relapse after ASCT | 5 (19) | 20 (25) |
| Grade ≥3 AEs* | ||
| Any grade ≥3 AE, n (%) | 27 (100) | 79 (98) |
| Neutropenia† | 20 (74) | 66 (81) |
| Anemia | 13 (48) | 36 (44) |
| Thrombocytopenia‡ | 12 (44) | 31 (38) |
| Decreased white blood cell count | 9 (33) | 22 (27) |
| Encephalopathy | 8 (30) | 17 (21) |
| Lymphocyte count decreased | 8 (30) | 14 (17) |
| Grade ≥3 infection | ||
| Infection, n (%) | 5 (19) | 25 (31) |
| Grade ≥3 CRS§ | ||
| Any grade ≥3 CRS, n (%) | 2 (7) | 10 (12) |
| Pyrexia | 3 (12) | 9 (12) |
| Hypotension | 2 (8) | 8 (11) |
| Hypoxia | 3 (12) | 6 (7) |
| Grade ≥3 neurologic event§ | ||
| Any grade ≥3 neurologic event, n (%) | 12 (44) | 23 (28) |
| Encephalopathy | 8 (30) | 17 (21) |
| Confusional state | 2 (7) | 8 (10) |
| Aphasia | 0 | 8 (10) |
| Agitation | 3 (11) | 2 (2) |
| Delirium | 3 (11) | 0 |
| Characteristic | ≥65 y (n = 27) | <65 y (n = 81) |
|---|---|---|
| Median age (range), y | 69 (65-76) | 55 (23-64) |
| Male, n (%) | 22 (81) | 51 (63) |
| ECOG performance status 1, n (%) | 16 (59) | 46 (57) |
| Disease stage III/IV, n (%) | 22 (81) | 68 (84) |
| IPI score 3-4, n (%) | 19 (70) | 29 (36) |
| ≥3 Prior therapies, n (%) | 18 (67) | 58 (72) |
| Median tumor burden by SPD (range), mm2 | 3 790 (600-16 764) | 3 574 (171-23 297) |
| Disease type, n (%) | ||
| DLBCL | 20 (74) | 64 (79) |
| PMBCL | 0 | 8 (10) |
| TFL | 7 (26) | 9 (11) |
| Prior ASCT, n (%) | 5 (19) | 24 (30) |
| Refractory subgroup before enrollment, n (%) | ||
| Primary refractory | 1 (4) | 2 (2) |
| Refractory to second-lineor later therapy | 21 (78) | 59 (73) |
| Relapse after ASCT | 5 (19) | 20 (25) |
| Grade ≥3 AEs* | ||
| Any grade ≥3 AE, n (%) | 27 (100) | 79 (98) |
| Neutropenia† | 20 (74) | 66 (81) |
| Anemia | 13 (48) | 36 (44) |
| Thrombocytopenia‡ | 12 (44) | 31 (38) |
| Decreased white blood cell count | 9 (33) | 22 (27) |
| Encephalopathy | 8 (30) | 17 (21) |
| Lymphocyte count decreased | 8 (30) | 14 (17) |
| Grade ≥3 infection | ||
| Infection, n (%) | 5 (19) | 25 (31) |
| Grade ≥3 CRS§ | ||
| Any grade ≥3 CRS, n (%) | 2 (7) | 10 (12) |
| Pyrexia | 3 (12) | 9 (12) |
| Hypotension | 2 (8) | 8 (11) |
| Hypoxia | 3 (12) | 6 (7) |
| Grade ≥3 neurologic event§ | ||
| Any grade ≥3 neurologic event, n (%) | 12 (44) | 23 (28) |
| Encephalopathy | 8 (30) | 17 (21) |
| Confusional state | 2 (7) | 8 (10) |
| Aphasia | 0 | 8 (10) |
| Agitation | 3 (11) | 2 (2) |
| Delirium | 3 (11) | 0 |
| Efficacy outcomes | ≥65 y (n = 24) | <65 y (n = 77) |
|---|---|---|
| Investigator-assessed ORR, n (%) | 22 (92) | 62 (81) |
| Complete response | 18 (75) | 41 (53) |
| Partial response | 4 (17) | 21 (27) |
| Ongoing response, n (%)ǁ | 10 (42) | 29 (38) |
| 24-Mo overall survival rate, % | 54 | 49 |
| Efficacy outcomes | ≥65 y (n = 24) | <65 y (n = 77) |
|---|---|---|
| Investigator-assessed ORR, n (%) | 22 (92) | 62 (81) |
| Complete response | 18 (75) | 41 (53) |
| Partial response | 4 (17) | 21 (27) |
| Ongoing response, n (%)ǁ | 10 (42) | 29 (38) |
| 24-Mo overall survival rate, % | 54 | 49 |
CRS, cytokine release syndrome; ECOG, Eastern Cooperative Oncology Group; PMBCL, primary mediastinal B-cell lymphoma; SPD, sum of product diameter; TFL, transformed follicular lymphoma.
Most common grade ≥3 AEs that occurred in ≥25% of either age group.
Neutropenia included the terms neutropenia, febrile neutropenia, and neutrophil count decreases.
Thrombocytopenia included the terms thrombocytopenia and platelet count decreases.
Symptoms shown are those that occurred in ≥10% of patients in either age group.
Patients in response as of the data cutoff.
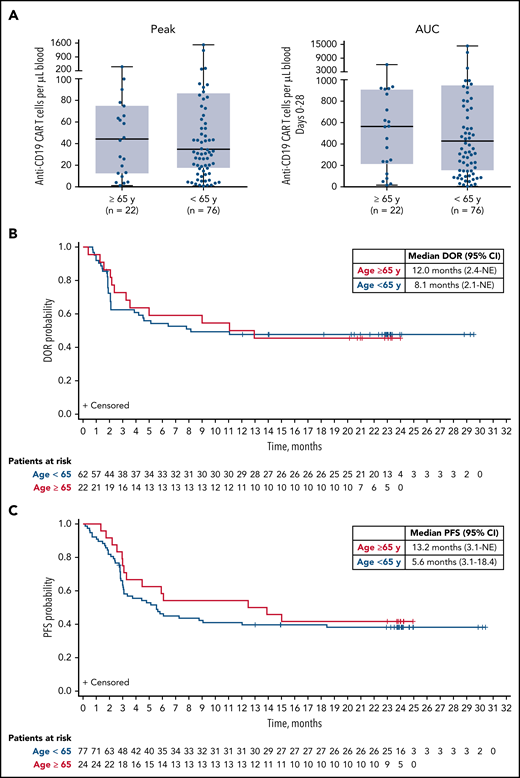
CAR T-cell expansion, DOR, and PFS by age group in ZUMA-1 phase 2 patients. (A) Peak levels (left) and AUC (days 0-28; right) of anti-CD19 CAR T cells per µL blood in patients ≥65 and <65 years of age. Phase 2 patients (n = 101) are shown. CAR T-cell levels were not available for 3 patients. (B) DOR among responders ≥65 and <65 years of age. (C) PFS in patients ≥65 and <65 years of age. AUC, area under the curve; CI, confidence interval; NE, not estimable.
CAR T-cell expansion, DOR, and PFS by age group in ZUMA-1 phase 2 patients. (A) Peak levels (left) and AUC (days 0-28; right) of anti-CD19 CAR T cells per µL blood in patients ≥65 and <65 years of age. Phase 2 patients (n = 101) are shown. CAR T-cell levels were not available for 3 patients. (B) DOR among responders ≥65 and <65 years of age. (C) PFS in patients ≥65 and <65 years of age. AUC, area under the curve; CI, confidence interval; NE, not estimable.
Adverse events (AEs) are summarized in Table 1. The most common grade ≥3 AEs were cytopenias, which occurred at similar rates in treated patients ≥65 and <65 years of age. The most common grade ≥3 cytopenia that was present on or after posttreatment day 93 was neutropenia, which was reported in 15% and 10% of patients ≥65 and <65 years of age, respectively. Rates of grade ≥3 cytokine release syndrome (CRS) were 7% for patients ≥65 and 12% for those <65 years of age. Grade ≥3 neurologic events were observed in 44% of patients ≥65 and 28% of those <65 years of age. Numerically higher rates of some neurologic event–associated symptoms were observed in patients ≥65 than in those <65 years of age, including grade ≥3 delirium and encephalopathy, which may be consistent with older age. Grade ≥3 infections were reported in 19% and 31% of patients ≥65 and <65 years of age, respectively. A total of 26% and 32% of patients ≥65 and <65 years of age, respectively, received intravenous immunoglobulin therapy at the discretion of the investigator. Grade 5 AEs were observed in 4 patients (4% of each age group), as previously reported.9-11 Our safety findings are consistent with those of a pooled analysis of 214 patients with large B-cell lymphoma enrolled in clinical trials of tisagenlecleucel and axi-cel, which reported comparable rates of grade ≥3 CRS in patients ≥65 and <65 years of age.12 Compared with this analysis of ZUMA-1, a subgroup analysis of 300 patients treated with axi-cel in the standard-of-care setting showed comparable rates of ORR and CRS, but modestly higher rates of complete response and all grade neurologic events, in patients ≥65 vs <65 years of age.13
In this subgroup analysis of the 2-year follow-up of ZUMA-1, axi-cel induced a high rate of durable responses with a manageable safety profile, regardless of age. No age-related differences in efficacy, pharmacokinetic profile, or safety were observed, suggesting that age alone should not limit axi-cel use. Overall, axi-cel demonstrated substantial clinical benefit for older patients with refractory large B-cell lymphoma, a population for whom treatment options are limited. Further analysis involving larger numbers of elderly patients treated with axi-cel as a standard-of-care therapy should be considered.14
Gilead is committed to sharing clinical trial data with external medical experts and scientific researchers in the interest of advancing public health. As such, Gilead shares anonymized individual patient data (IPD) upon request or as required by law and/or regulation. Qualified external researchers may request IPD for studies of Gilead compounds approved in the United States and the European Union with a marketing authorization date on or after 1 January 2014 and are publicly listed on clinicaltrials.gov or the European Union-Clinical Trials Register (EU CTR). For studies of newly approved compounds or indication, the IPD will be available for request 6 months after US Food and Drug Administration (FDA) and European Medicines Agency (EMA) approval. Such requests are at Gilead’s discretion and are dependent on the nature of the request, the merit of the research proposed, availability of the data, and the intended use of the data. If Gilead agrees to the release of clinical data for research purposes, the requestor will be required to sign a data sharing agreement, to ensure protection of patient confidentiality before the release of any data.
Presented in poster form at the annual meeting of the American Society of Clinical Oncology, Chicago, IL, 3 June 2019
The online version of this article contains a data supplement.
Acknowledgments
The authors thank the patients; their families, friends, and caregivers; and all study staff and health care providers who participated in this study.
This work was supported by Kite, a Gilead Company, and the Leukemia and Lymphoma Society Therapy Acceleration Program. Medical writing support was provided by Jennifer Leslie, of Nexus Global Group Science, with funding from Kite.
Authorship
Contribution: S.S.N. and F.L.L. designed the study; S.S.N., C.A.J., D.B.M., O.O.O., I.B., A.D., J.M., N.L.B., and F.L.L. enrolled and treated patients and gathered data; S.S.N., Y.J., L.Z., J.M.R., J.J.K., and F.L.L. analyzed and interpreted data; and all authors participated in writing the article, provided feedback throughout the development process, and approved the final submitted version.
Conflict-of-interest disclosure: S.S.N. has received personal fees from Kite, Merck, Novartis, Celgene, Pfizer, Allogene, Cell Medica, Incyte, Precision Biosciences, Legend Biotech, and Unum Therapeutics and research support from Kite, Bristol-Myers Squibb, Merck, Poseida, Cellectis, Celgene, Karus Therapeutics, Unum Therapeutics, Allogene, and Acerta. C.A.J. has received personal fees from Kite, Novartis, Precision Bioscience, Bayer, Pfizer, and Humanigen. J.M. has served in a consultancy or advisory role for Genentech, Alexion, Bayer, Bristol-Myers Squibb, Juno/Celgene, Kite, Kyowa, Merck, Pfizer, Pharmacyclics/Janssen, and Seattle Genetics; has served on speakers’ bureaus for AstraZeneca, Bayer, Fosunkite, Genentech, Kite, Kyowa, Pharmacyclics/Janssen, and Seattle Genetics; and has received research funding from Celgene, Genentech, Incyte, Janssen, Kite, Pharmacyclics, Portola, and Seattle Genetics. A.D. has served on advisory boards for Kite, Agios, and Novartis and has received research funding from Bristol-Myers Squibb. D.B.M has received grants and research funding from and served on a scientific advisory board for Kite. N.L.B has received research funding from Affimed, Bristol-Myers Squibb, Celgene, Forty Seven, Genentech, Gilead, Immune Design, Kite, Merck, Millennium, and Pharmacyclics and serves on advisory boards for Acerta and ADC Therapeutics. I.B. has received speaker fees from Kite. Y.J., J.J.K., L.Z., and J.M.R. are employees of Kite and have equity ownership in Gilead Sciences Inc. F.L.L has been a scientific advisor to Kite, Novartis, and GammaDelta Therapeutics and is a consultant for Cellular Biomedicine Group Inc. The remaining authors declare no competing financial interests.
Correspondence: Sattva S. Neelapu, The University of Texas MD Anderson Cancer Center, Unit 429, 1515 Holcombe Blvd, Houston, TX 77030; e-mail: sneelapu@mdanderson.org.
