

Key Points
The Janus kinase (JAK)1/2 inhibitor ruxolitinib induced responses in more than half of patients with steroid-refractory aGVHD by day 28.
Ruxolitinib was well tolerated, and the safety profile was consistent with expectations for ruxolitinib and this patient population.

Abstract
Patients who develop steroid-refractory acute graft-versus-host disease (aGVHD) after allogeneic hematopoietic cell transplantation have poor prognosis, highlighting an unmet therapeutic need. In this open-label phase 2 study (ClinicalTrials.gov identifier: NCT02953678), patients aged at least 12 years with grades II to IV steroid-refractory aGVHD were eligible to receive ruxolitinib orally, starting at 5 mg twice daily plus corticosteroids, until treatment failure, unacceptable toxicity, or death. The primary end point was overall response rate (ORR) at day 28; the key secondary end point was duration of response (DOR) at 6 months. As of 2 July 2018, 71 patients received at least 1 dose of ruxolitinib. Forty-eight of those patients (67.6%) had grade III/IV aGVHD at enrollment. At day 28, 39 patients (54.9%; 95% confidence interval, 42.7%-66.8%) had an overall response, including 19 (26.8%) with complete responses. Best ORR at any time was 73.2% (complete response, 56.3%). Responses were observed across skin (61.1%), upper (45.5%) and lower (46.0%) gastrointestinal tract, and liver (26.7%). Median DOR was 345 days. Overall survival estimate at 6 months was 51.0%. At day 28, 24 (55.8%) of 43 patients receiving ruxolitinib and corticosteroids had a 50% or greater corticosteroid dose reduction from baseline. The most common treatment-emergent adverse events were anemia (64.8%), thrombocytopenia (62.0%), hypokalemia (49.3%), neutropenia (47.9%), and peripheral edema (45.1%). Ruxolitinib produced durable responses and encouraging survival compared with historical data in patients with steroid-refractory aGVHD who otherwise have dismal outcomes. The safety profile was consistent with expectations for ruxolitinib and this patient population.
Introduction
Allogeneic hematopoietic cell transplantation (HCT) is a potentially curative treatment option for a variety of hematologic malignancies and several nonmalignant hematologic diseases.1,2 More than 8000 HCT procedures have been performed annually in the United States since 2013, with acute myeloid leukemia, myelodysplastic syndrome/myeloproliferative disorders, and acute lymphoblastic leukemia representing the most common indications.2 Acute graft-versus-host disease (aGVHD) develops in 50% to 70% of patients after HCT with conventional prophylaxis, and is one of the major barriers to successful transplant outcomes.3,4
The pathogenesis of aGVHD is complex and is initiated when alloreactive donor immune cells recognize immunologically disparate antigens in the host.1,5 T-cell receptor activation of donor T cells plays a critical role in aGVHD, and the subsequent immune response against the host results in tissue damage, primarily in the skin, liver, and gut.1,5 The risk of developing aGVHD depends on the degree of HLA match, recipient age, graft source, underlying disease diagnosis, and intensity of conditioning regimen and GVHD prophylaxis used.3,6 Systemic corticosteroids are the recommended first-line treatment of grades II to IV aGVHD, but less than 50% of patients achieve durable responses.7,8 The reported 6-month survival estimate for patients with steroid-refractory aGVHD is approximately 50%, with 30% or less of patients surviving beyond 2 years.8-10 Ruxolitinib recently became the first drug approved by the US Food and Drug Administration for the treatment of steroid-refractory aGVHD in adults and pediatric patients aged 12 years and older.11
Ruxolitinib is an oral, selective inhibitor of Janus kinase (JAK)1/2. JAKs are intracellular tyrosine kinases that play a critical role in the development and function of immune cells, and have been implicated in aGVHD pathogenesis.12 Retrospective clinical studies of ruxolitinib as salvage therapy for steroid-refractory aGVHD suggest clinical benefit, including encouraging overall survival (OS) rates.13-15
REACH1 is the first prospective clinical trial evaluating the efficacy and safety of ruxolitinib for the treatment of patients with steroid-refractory aGVHD. Here we report efficacy and safety results after 6 months of follow-up.
Methods
Study design and patients
REACH1 is a prospective, multicenter, open-label, single-cohort, phase 2 trial (ClinicalTrials.gov identifier: NCT02953678) recruiting patients at 26 medical centers across 17 US states. Eligible patients were aged at least 12 years, had undergone their first HCT from any donor source for hematologic malignancies, had evidence of myeloid engraftment, developed clinically suspected grades II to IV steroid-refractory aGVHD per Mount Sinai Acute GVHD International Consortium (MAGIC) criteria,16 and received no more than 1 systemic treatment in addition to corticosteroids for treatment of aGVHD. Patients with prior infection were eligible to participate, provided they did not have an active, uncontrolled infection at screening. Steroid-refractory aGVHD was defined as progressive GVHD after 3 days or no improvement of GVHD after 7 days of primary treatment with at least 2 mg/kg per day methylprednisolone (or equivalent), development of new organ GVHD after lower-dose corticosteroid treatment (≥1 mg/kg per day methylprednisolone) for skin or skin plus upper gastrointestinal (GI) GVHD, or inability to tolerate corticosteroid taper (supplemental Table 1, available on the Blood Web site, contains full eligibility criteria).
The protocol was approved by institutional review boards at participating centers. The full study protocol is available in the supplemental Appendix. The study was conducted in accordance with the International Council for Harmonization Guideline for Good Clinical Practice and the principles embodied by the Declaration of Helsinki. All patients provided written informed consent. Incyte Corporation sponsored the REACH1 trial, participated in study design development, and collaborated with authors in analyzing and interpreting the data and writing the manuscript. All authors had full access to the study data.
Procedures
Patients received a starting oral dose of ruxolitinib at 5 mg twice daily (based on guidance from the US Food and Drug Administration), with an option to increase to 10 mg twice daily after 3 days in the absence of cytopenias (≥50% decrease in platelet counts and/or absolute neutrophil count relative to day 1). Ruxolitinib could be tapered after day 180 in patients who achieved complete response (CR) or very good partial response (VGPR) and had discontinued corticosteroids for at least 8 weeks. The starting dose of corticosteroids was methylprednisolone 2.0 mg/kg per day intravenously or prednisone 2.5 mg/kg per day orally on day 1; corticosteroids were tapered per institutional guidelines. Patients who previously began corticosteroids at a different dose than the recommended starting dose (methylprednisolone 2.0 mg/kg per day intravenously or prednisone 2.5 mg/kg per day orally) were permitted to remain on that dose at the treating physicians’ discretion. Patients who experienced GVHD flares during corticosteroid taper could continue receiving ruxolitinib. Continued use of prophylactic antibiotic, antiviral, and antifungal medications was permitted throughout the study at the discretion of the investigator. Patients received study treatment until treatment failure, unacceptable toxicity, withdrawal of consent, or death.
End points
The primary end point was overall response rate (ORR) at day 28, defined as the proportion of patients demonstrating a CR, VGPR, or partial response (PR).17 The key secondary end point was duration of response (DOR; time from first response to GVHD progression or death), which was calculated once all patients reached 6 months. Additional secondary end points included ORR at any time, nonrelapse mortality (NRM), relapse rate, OS, chronic GVHD (cGVHD), safety, and pharmacokinetics. Exploratory end points included average corticosteroid dose and biomarkers.
Acute GVHD was graded by the investigator per MAGIC guidelines.16 Response was assessed as previously described.17,18 Patients were evaluated for cGVHD signs and symptoms per National Institutes of Health consensus guidelines.19 Adverse events (AEs) were assessed according to National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) v.4.03. Additional details on trial end points and assessments are provided in the supplemental Appendix.
Statistical analysis
The targeted ORR at day 28 was 60%. With a sample size of 70 patients, the study had 90% power to exclude a lower 95% confidence limit of 40%. The ORR at day 28 (primary end point) and at various times was calculated, together with its 95% confidence interval (CI). Kaplan-Meier methodology was used to estimate DOR and OS. A post hoc multivariate analysis of baseline characteristics and response at day 28 was performed using logistic regression. Post hoc model-based analyses of baseline characteristics with OS and NRM were performed using Cox regression and Fine and Gray regression, respectively. For the post hoc OS analysis, HLA matching, aGVHD grade at enrollment, steroid-refractory status, and duration of prior corticosteroid exposure were assessed as covariates.
All patients enrolled in the study were included in the efficacy analysis; patients who received at least 1 dose of ruxolitinib were included in the safety analysis. Reduction in corticosteroid use was assessed at day 28 in patients who were still receiving ruxolitinib treatment because corticosteroid dosage data collected after ruxolitinib discontinuation may be unreliable and patients may have received additional medications. The data cutoff for this analysis was 2 July 2018.
Results
Patients
Between 27 December 2016 and 2 July 2018, 71 patients received at least 1 dose of ruxolitinib. Median age was 58 (range, 18-73) years, and 48 patients (67.6%) had grade III/IV aGVHD at enrollment (Table 1). Median exposure to corticosteroids for all patients before enrollment was 15 (range, 3-285) days (Table 1) and 17 and 12 days for patients with grade II and grade III/IV aGVHD, respectively. No patients had chronic GVHD or overlap syndrome at the time of enrollment. Table 2 presents prior corticosteroid use by steroid-refractory aGVHD status. All patients received anti-infective prophylaxis: 83.1% received triazole derivatives, 97.2% received nucleosides/nucleotides (excluding reverse transcription inhibitors), and 59.2% received antimycotics before or during the study (supplemental Table 2). At the time of the analysis, 30 patients (42.3%) remained on study and 11 (15.5%) were receiving ruxolitinib. The median follow-up interval was 156.0 (range, 9-518) days. Reasons for ruxolitinib discontinuation were AEs (28.2%), physician decision (28.2%; including 4 patients who had clinical improvement), death (9.9%), and aGVHD progression (8.5%; supplemental Figure 1).
Patient demographics and baseline disease characteristics
| Variable | Ruxolitinib (N = 71) |
|---|---|
| Median (range) age, y | 58 (18-73) |
| Age group, n (%) | |
| <65 y | 58 (81.7) |
| ≥65 y | 13 (18.3) |
| Female, n (%) | 36 (50.7) |
| Race, n (%) | |
| White | 66 (93.0) |
| Black | 3 (4.2) |
| Asian | 2 (2.8) |
| MAGIC aGVHD grade, n (%) | |
| II | 23 (32.4) |
| III | 34 (47.9) |
| IV | 14 (19.7) |
| Steroid-refractory criteria, n (%) | |
| Progressive GVHD after 3 d of primary treatment | 19 (26.8) |
| GVHD not improved after 7 d of primary treatment | 30 (42.3) |
| Previously began CS therapy at a lower dose, but developed new GVHD in another organ system | 8 (11.3) |
| Unable to tolerate CS taper | 14 (19.7) |
| Median (range) prior exposure to corticosteroids, d | 15 (3-285) |
| Underlying malignancy, n (%) | |
| Acute myeloid leukemia | 20 (28.2) |
| Myelodysplastic syndrome | 20 (28.2) |
| Lymphoma | 9 (12.7) |
| Acute lymphoblastic leukemia | 8 (11.3) |
| Chronic lymphocytic leukemia | 3 (4.2) |
| Myelofibrosis/myeloproliferative neoplasm | 2 (2.8) |
| Multiple myeloma | 2 (2.8) |
| Other | 7 (9.9) |
| Donor type, n (%) | |
| Matched unrelated donor | 27 (38.0) |
| Matched related donor | 18 (25.4) |
| Mismatched related donor | 11 (15.5) |
| Mismatched unrelated donor | 10 (14.1) |
| Other | 5 (7.0) |
| Conditioning regimen, n (%) | |
| Nonmyeloablative | 36 (50.7) |
| Myeloablative | 31 (43.7) |
| Missing | 4 (5.6) |
| Prior lines of therapy (other than corticosteroids), n (%) | |
| 1 | 59 (83.1) |
| >1 | 12 (16.9) |
| Graft type, n (%) | |
| Peripheral blood stem cells | 57 (80.3) |
| Bone marrow | 13 (18.3) |
| Umbilical cord blood | 1 (1.4) |
| CMV serostatus, n (%)* | |
| Donor-positive/recipient-positive | 24 (33.8) |
| Donor-positive/recipient-negative | 7 (9.9) |
| Donor-negative/recipient-positive | 16 (22.5) |
| Donor-negative/recipient-negative | 23 (32.4) |
| Missing | 1 (1.4) |
| Variable | Ruxolitinib (N = 71) |
|---|---|
| Median (range) age, y | 58 (18-73) |
| Age group, n (%) | |
| <65 y | 58 (81.7) |
| ≥65 y | 13 (18.3) |
| Female, n (%) | 36 (50.7) |
| Race, n (%) | |
| White | 66 (93.0) |
| Black | 3 (4.2) |
| Asian | 2 (2.8) |
| MAGIC aGVHD grade, n (%) | |
| II | 23 (32.4) |
| III | 34 (47.9) |
| IV | 14 (19.7) |
| Steroid-refractory criteria, n (%) | |
| Progressive GVHD after 3 d of primary treatment | 19 (26.8) |
| GVHD not improved after 7 d of primary treatment | 30 (42.3) |
| Previously began CS therapy at a lower dose, but developed new GVHD in another organ system | 8 (11.3) |
| Unable to tolerate CS taper | 14 (19.7) |
| Median (range) prior exposure to corticosteroids, d | 15 (3-285) |
| Underlying malignancy, n (%) | |
| Acute myeloid leukemia | 20 (28.2) |
| Myelodysplastic syndrome | 20 (28.2) |
| Lymphoma | 9 (12.7) |
| Acute lymphoblastic leukemia | 8 (11.3) |
| Chronic lymphocytic leukemia | 3 (4.2) |
| Myelofibrosis/myeloproliferative neoplasm | 2 (2.8) |
| Multiple myeloma | 2 (2.8) |
| Other | 7 (9.9) |
| Donor type, n (%) | |
| Matched unrelated donor | 27 (38.0) |
| Matched related donor | 18 (25.4) |
| Mismatched related donor | 11 (15.5) |
| Mismatched unrelated donor | 10 (14.1) |
| Other | 5 (7.0) |
| Conditioning regimen, n (%) | |
| Nonmyeloablative | 36 (50.7) |
| Myeloablative | 31 (43.7) |
| Missing | 4 (5.6) |
| Prior lines of therapy (other than corticosteroids), n (%) | |
| 1 | 59 (83.1) |
| >1 | 12 (16.9) |
| Graft type, n (%) | |
| Peripheral blood stem cells | 57 (80.3) |
| Bone marrow | 13 (18.3) |
| Umbilical cord blood | 1 (1.4) |
| CMV serostatus, n (%)* | |
| Donor-positive/recipient-positive | 24 (33.8) |
| Donor-positive/recipient-negative | 7 (9.9) |
| Donor-negative/recipient-positive | 16 (22.5) |
| Donor-negative/recipient-negative | 23 (32.4) |
| Missing | 1 (1.4) |
CS, corticosteroid.
Donor serostatus was missing from 1 patient (patient was positive).
Prior corticosteroid use by steroid-refractory status
| GVHD progression after 3 d* (n = 19) | No improvement in GVHD after 7 d* (n = 30) | New GVHD† (n = 8) | Taper intolerant (n = 14) | Total (N = 71) | |
|---|---|---|---|---|---|
| Dose of corticosteroid at enrollment, mg/d | |||||
| Mean (SD) | 179.9 (58.1) | 169.9 (63.5) | 114.2 (55.0) | 124.1 (45.9) | 157.3 (62.2) |
| Median (range) | 180.0 (81.3-300.0) | 168.8 (62.5-300.0) | 109.4 (50.0-212.5) | 125.0 (60.0-200.0) | 156.3 (50.0-300.0) |
| Days on corticosteroids before enrollment | |||||
| Mean (SD) | 31.6 (52.8) | 32.2 (54.9) | 20.6 (23.5) | 28.9 (23.4) | 30.1 (46.2) |
| Median (range) | 14.0 (6.0-224.0) | 13.0 (6.0-285.0) | 13.5 (3.0-75.0) | 21.0 (6.0-85.0) | 15.0 (3.0-285.0) |
| GVHD progression after 3 d* (n = 19) | No improvement in GVHD after 7 d* (n = 30) | New GVHD† (n = 8) | Taper intolerant (n = 14) | Total (N = 71) | |
|---|---|---|---|---|---|
| Dose of corticosteroid at enrollment, mg/d | |||||
| Mean (SD) | 179.9 (58.1) | 169.9 (63.5) | 114.2 (55.0) | 124.1 (45.9) | 157.3 (62.2) |
| Median (range) | 180.0 (81.3-300.0) | 168.8 (62.5-300.0) | 109.4 (50.0-212.5) | 125.0 (60.0-200.0) | 156.3 (50.0-300.0) |
| Days on corticosteroids before enrollment | |||||
| Mean (SD) | 31.6 (52.8) | 32.2 (54.9) | 20.6 (23.5) | 28.9 (23.4) | 30.1 (46.2) |
| Median (range) | 14.0 (6.0-224.0) | 13.0 (6.0-285.0) | 13.5 (3.0-75.0) | 21.0 (6.0-85.0) | 15.0 (3.0-285.0) |
After primary treatment with methylprednisolone at least 2 mg/kg per day.
In another organ in patients who previously received corticosteroids (≥1 mg/kg per day methylprednisolone) for skin or skin plus upper GI GVHD.
Response outcomes
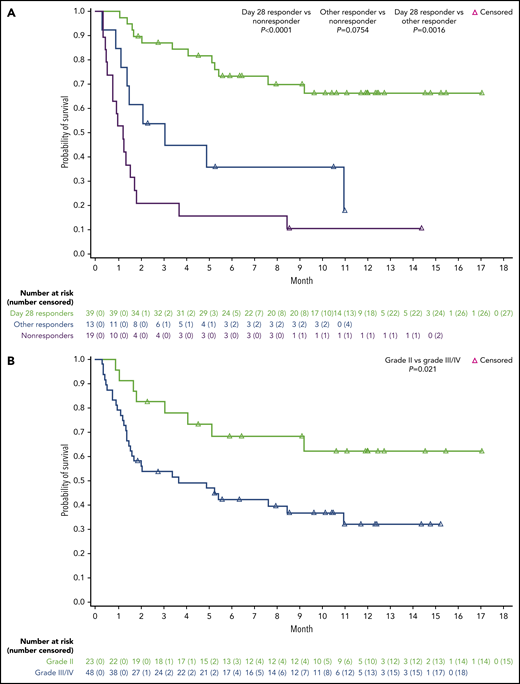
The median duration of ruxolitinib treatment of all patients was 46 (range, 4-473) days, and the median average total daily dose was 10.3 (range, 5-20) mg/d. The primary end point, overall response at day 28, was observed for 39 patients (54.9%; 95% CI, 42.7%-66.8%), including 19 patients (26.8%) with CR, 7 (9.9%) with VGPR, and 13 (18.3%) with PR (Table 3). The median DOR at 6 months was 345 days (lower limit, 159 days; Figure 1A).
ORR at day 28 by baseline aGVHD grade
| Response | Grade II (n = 23) | Grade III (n = 34) | Grade IV (n = 14) | Total (N =71) |
|---|---|---|---|---|
| CR | 11 (47.8) | 7 (20.6) | 1 (7.1) | 19 (26.8) |
| VGPR | 4 (17.4) | 2 (5.9) | 1 (7.1) | 7 (9.9) |
| PR | 4 (17.4) | 5 (14.7) | 4 (28.6) | 13 (18.3) |
| Overall response | 19 (82.6) | 14 (41.2) | 6 (42.9) | 39 (54.9) |
| 95% CI | 61.2-95.0 | 24.6-59.3 | 17.7-71.1 | 42.7-66.8 |
| Response | Grade II (n = 23) | Grade III (n = 34) | Grade IV (n = 14) | Total (N =71) |
|---|---|---|---|---|
| CR | 11 (47.8) | 7 (20.6) | 1 (7.1) | 19 (26.8) |
| VGPR | 4 (17.4) | 2 (5.9) | 1 (7.1) | 7 (9.9) |
| PR | 4 (17.4) | 5 (14.7) | 4 (28.6) | 13 (18.3) |
| Overall response | 19 (82.6) | 14 (41.2) | 6 (42.9) | 39 (54.9) |
| 95% CI | 61.2-95.0 | 24.6-59.3 | 17.7-71.1 | 42.7-66.8 |
Data are presented as n (%).

Response outcomes. (A) Duration of response (time from first response until GVHD progression or death) in day 28 responders and other responders (patients who responded at any time during treatment). The data cutoff was 2 July 2018. (B) Subgroup analysis of day 28 ORR. Acute GVHD response was assessed using standardized objective criteria per MAGIC guidelines. *After primary treatment with methylprednisolone ≥2 mg/kg per day. †In another organ in patients who previously received corticosteroids (≥1 mg/kg per day methylprednisolone) for skin or skin plus upper GI GVHD.
Response outcomes. (A) Duration of response (time from first response until GVHD progression or death) in day 28 responders and other responders (patients who responded at any time during treatment). The data cutoff was 2 July 2018. (B) Subgroup analysis of day 28 ORR. Acute GVHD response was assessed using standardized objective criteria per MAGIC guidelines. *After primary treatment with methylprednisolone ≥2 mg/kg per day. †In another organ in patients who previously received corticosteroids (≥1 mg/kg per day methylprednisolone) for skin or skin plus upper GI GVHD.
The ORR at any time was 73.2% (95% CI, 61.4%-83.1%; CR, 56.3%), which included 9 patients (12.7%) who had a response (2 CR, 1 VGPR, 6 PR) before day 28 but did not respond at the day 28 visit, and 4 patients (5.6%) who responded after day 28 (1 CR, 3 PR). The median time to first response was 7 (range, 6-49) days; 43 patients (60.6%) had first response on or before the day 14 visit. The median DOR at 6 months for patients with a response at any time was also 345 days (lower limit, 106 days).
Subgroup analysis of baseline characteristics demonstrated that day 28 response was associated with aGVHD grade at enrollment; no significant associations were observed for other factors evaluated (Figure 1B). Responses were observed irrespective of steroid-refractory status (Table 4) and across skin (61.1%), upper (45.5%) and lower (46.0%) GI tract, and liver (26.7%; Table 5; Figure 1B). Day 28 response rates were 62.9% and 47.2% among patients with 1 organ and 2 or more organs involved at enrollment, respectively. In a post hoc model-based analysis, grade II vs. grade III/IV aGVHD was significantly associated with day 28 response (odds ratio, 0.15; 95% CI, 0.04-0.55; P = .0042).
ORR at day 28 by baseline steroid-refractory status
| Response | GVHD progression after 3 d* (n = 19) | No improvement in GVHD after 7 d* (n = 30) | New GVHD† (n = 8) | Taper intolerant (n = 14) |
|---|---|---|---|---|
| CR | 7 (36.8) | 6 (20.0) | 1 (12.5) | 5 (35.7) |
| VGPR | 4 (21.1) | 1 (3.3) | 1 (12.5) | 1 (7.1) |
| PR | 1 (5.3) | 7 (23.3) | 2 (25.5) | 3 (21.4) |
| Overall response | 12 (63.2) | 14 (46.7) | 4 (50.0) | 9 (64.3) |
| 95% CI | 38.4-83.7 | 28.3-65.7 | 15.7-84.3 | 35.1-87.2 |
| Response | GVHD progression after 3 d* (n = 19) | No improvement in GVHD after 7 d* (n = 30) | New GVHD† (n = 8) | Taper intolerant (n = 14) |
|---|---|---|---|---|
| CR | 7 (36.8) | 6 (20.0) | 1 (12.5) | 5 (35.7) |
| VGPR | 4 (21.1) | 1 (3.3) | 1 (12.5) | 1 (7.1) |
| PR | 1 (5.3) | 7 (23.3) | 2 (25.5) | 3 (21.4) |
| Overall response | 12 (63.2) | 14 (46.7) | 4 (50.0) | 9 (64.3) |
| 95% CI | 38.4-83.7 | 28.3-65.7 | 15.7-84.3 | 35.1-87.2 |
Data are presented as n (%).
After primary treatment with methylprednisolone at least 2 mg/kg per day.
In another organ in patients who previously received corticosteroids (≥1 mg/kg per day methylprednisolone) for skin or skin plus upper GI GVHD.
ORR at day 28 by baseline organ involvement
| Response | Skin (n = 36) | Liver (n = 15) | Upper GI (n = 22) | Lower GI (n = 50) |
|---|---|---|---|---|
| CR | 9 (25.0) | 2 (13.3) | 5 (22.7) | 12 (24.0) |
| VGPR | 6 (16.7) | 0 | 0 | 3 (6.0) |
| PR | 7 (19.4) | 2 (13.3) | 5 (22.7) | 8 (16.0) |
| Overall response | 22 (61.1) | 4 (26.7) | 10 (45.5) | 23 (46.0) |
| 95% CI | 43.5-76.9 | 7.8-55.1 | 24.4-67.8 | 31.8-60.7 |
| Response | Skin (n = 36) | Liver (n = 15) | Upper GI (n = 22) | Lower GI (n = 50) |
|---|---|---|---|---|
| CR | 9 (25.0) | 2 (13.3) | 5 (22.7) | 12 (24.0) |
| VGPR | 6 (16.7) | 0 | 0 | 3 (6.0) |
| PR | 7 (19.4) | 2 (13.3) | 5 (22.7) | 8 (16.0) |
| Overall response | 22 (61.1) | 4 (26.7) | 10 (45.5) | 23 (46.0) |
| 95% CI | 43.5-76.9 | 7.8-55.1 | 24.4-67.8 | 31.8-60.7 |
Data are presented as n (%).
OS and nonrelapse mortality
The 6- and 12-month OS rates for all patients were 51.0% (95% CI, 38.7%-62.1%) and 42.6% (95% CI, 30.0%-54.6%), respectively; median OS was 7.6 (95% CI, 3.1: not evaluable) months. OS was greater for day 28 responders compared with nonresponders (P < .0001) or other responders (P = .0016; Figure 2A). The probability that day 28 responders were alive at 6 and 12 months was 73.2% (95% CI, 55.9%-84.6%) and 66.2% (95% CI, 47.8%-79.4%), respectively. In a model-based analysis of OS, aGVHD grade III/IV and longer prior corticosteroid exposure were significantly associated with reduced OS (grade III/IV aGVHD, P = .0076 [Figure 2B]; duration of prior corticosteroid exposure, hazard ratio [HR], 1.01; 95% CI, 1.00-1.02; P = .0015). Response status, when added to the model, was an independent predictor of OS (HR, 0.40; 95% CI, 0.26-0.61; P < .0001).
OS and NRM. (A) Kaplan-Meier estimates of OS in patients by response status (day 28 responders, other responders, nonresponders). OS was defined as the time from first ruxolitinib treatment to death for any cause. The data cutoff was 2 July 2018. (B) OS by aGVHD grade at enrollment. aGVHD grade at enrollment was significantly associated with OS by log-rank test in the Kaplan-Meier analysis (P = .021). In model-based analysis of OS by Cox regression, aGVHD grade III/IV was again significantly associated with reduced OS (aGVHD grade III/IV vs grade II [reference]; HR, 0.334; 95% CI, 0.150-0.747; P = .0076). (C) NRM by response status. The 6-month cumulative incidence rate for NRM was 44.4% (95% CI, 32.5%-55.7%) for the entire patient cohort, 21.2% (95% CI, 9.9%-35.2%) for day 28 responders, 64.1% (95% CI, 31.5%-84.3%) for other responders, and 78.9% (95% CI, 53.2%-91.5%) for nonresponders. The 12-month cumulative incidence rate for NRM was 52.9% (95% CI, 39.6%-64.5%) for all patients, 28.2% (95% CI, 14.5%-43.6%) for day 28 responders, and 84.2% (95% CI, 58.7%-94.6%) for nonresponders. The 12-month NRM rate for other responders was not evaluable.

Causes of death
Thirty-five patients (49.3%) died of causes other than malignancy relapse, including 10 patients who died within the first 28 days. The 6- and 12-month cumulative incidence rates for NRM were 44.4% (95% CI, 32.5%-55.7%) and 52.9% (95% CI, 39.6%-64.5%), respectively, for all patients, and were lower for day 28 responders (Figure 2C). Four patients (5.6%) had a malignancy relapse (acute myeloid leukemia, n = 2 [both fatal]; myelodysplastic syndrome, n = 1; plasma cell leukemia, n = 1 [fatal]). All relapses occurred on the day of (n = 2) or after (n = 2; 34 days and 99 days from last dose) ruxolitinib discontinuation. Mortality outcomes by response status are provided in supplemental Figure 2. In a model-based analysis of NRM using the same covariates as in OS, aGVHD grade III/IV (HR, 0.252; 95% CI, 0.11-0.58; P = .0013) and longer prior corticosteroid exposure (HR, 1.01; 95% CI, 1.01-1.02; P = .0001) were significantly associated with increased NRM. When added to the model, response status was an independent predictor of NRM (HR, 0.442; 95% CI, 0.29-0.69; P = .0003).
Supplemental Table 3 describes outcomes (ORR, OS, DOR, NRM) stratified by aGVHD grade at enrollment (grade II vs III/IV) and response (CR/VGPR vs PR). Of the 48 patients with grade III/IV aGVHD, 11 (22.9%) achieved CR or VGPR at day 28. Among the 11 patients with CR or VGPR, OS probability was 81.8% and NRM cumulative incidence rate was 9.1% at both 6 and 12 months. The relationship between skin vs nonskin involvement at enrollment and response was also explored. Patients with grade II and grade III/IV aGVHD at enrollment with skin involvement had day 28 ORRs of 88.2% and 36.8%, respectively. Patients with grade II and grade III/IV aGVHD without skin involvement had day 28 ORRs of 66.7% and 44.8%, respectively.
Long-term follow-up
At a median follow-up of 323 (range, 57-518) days for surviving patients, 4 patients developed cGVHD after discontinuation of ruxolitinib (on study days 55, 115, 156, and 347).
Pharmacokinetics
Covariate analysis was performed to identify factors predictive of variability in ruxolitinib pharmacokinetics in patients with aGVHD. In addition to effects of body weight on apparent central volume of distribution and sex on apparent oral clearance (CL/F) of ruxolitinib, concomitant use of moderate or potent cytochrome P450 3A4 (CYP3A4) inhibitors, grade IV aGVHD, and liver involvement were predictive of variability in CL/F. Acute GVHD grade (grade 0-I vs ≥II) was the only significant predictor of first-order absorption rate constant.
Corticosteroid use
The median initial corticosteroid dose (methylprednisolone dose [mg] × 1.25 = prednisone dose [mg]) after the start of ruxolitinib treatment was 156.3 mg/d. By day 28, the median average daily corticosteroid dose per patient was 62.5 mg/d, and 55.8% (24/43) of patients receiving ruxolitinib had a 50% or more reduction from baseline corticosteroid dose (Figure 3).
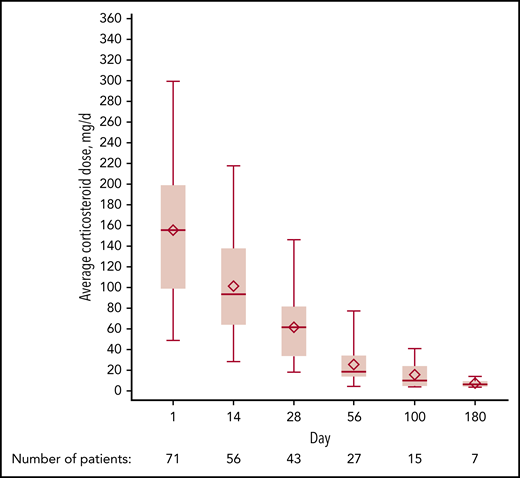
Average corticosteroid dose over time. The average corticosteroid dose in milligrams per day at days 1, 14, 28, 56, 100, and 180 is displayed for patients who continued receiving ruxolitinib treatment. Data shown indicate median (horizontal line), mean (diamond), 75th and 25th quartiles (upper and lower boundaries, respectively), and minimum (lower error bar)/maximum (upper error bar).
Average corticosteroid dose over time. The average corticosteroid dose in milligrams per day at days 1, 14, 28, 56, 100, and 180 is displayed for patients who continued receiving ruxolitinib treatment. Data shown indicate median (horizontal line), mean (diamond), 75th and 25th quartiles (upper and lower boundaries, respectively), and minimum (lower error bar)/maximum (upper error bar).
Biomarker analyses
A prespecified biomarker analysis explored potential predictive and correlative biomarkers based on patients’ day 28 response. Baseline levels of suppression of tumorigenicity 2 (ST2) and tumor necrosis factor receptor 1 (TNFR1), but not regenerating islet-derived protein 3α (REG3A) or Trappin-2/Elafin, were significantly elevated in nonresponders compared with responders (supplemental Table 4; supplemental Figure 3). Broad proteomic analysis revealed that among day 28 responders, 60 proteins primarily associated with hematopoiesis pathways were significantly upregulated after ruxolitinib treatment and 19 proteins primarily associated with interleukin (IL)-17–mediated inflammation were downregulated (supplemental Tables 5 and 6; supplemental Figure 4).
Safety
All patients had at least 1 treatment-emergent AE (TEAE); 69 patients (97.2%) had a grade 3 or higher TEAE. AEs led to ruxolitinib discontinuation, dose reduction, and dose interruption in 23 (32.4%), 25 (35.2%), and 29 (40.8%) patients, respectively. TEAEs occurring in 10% or more of patients are provided in supplemental Table 7. Thrombotic microangiopathy was reported in 2 patients (2.8%). The most common hematologic TEAEs were anemia (64.8%), thrombocytopenia (62.0%), and neutropenia (47.9%). Infections occurred in 57 patients (80.3%); the most frequent were cytomegalovirus (CMV) events (19.7%; CMV infection, 12.7%; CMV viremia, 5.6%; retinitis, 1.4%), sepsis (12.7%), and bacteremia (9.9%). All patients who had a CMV event had a positive CMV donor or recipient serostatus or both at baseline (supplemental Table 8). Supplemental Table 3 describes CTCAE grade 4 infections stratified by grade II vs grade III/IV aGVHD.
Fifty-three patients (74.6%) had at least 1 AE deemed related to ruxolitinib, with the most common being anemia (35.2%), decreased platelet count (32.4%), and decreased neutrophil count (26.8%; Table 6). Two patients had fatal TEAEs (pulmonary hemorrhage and sepsis [n = 1, each]) that were considered related to both ruxolitinib and corticosteroids.
Ruxolitinib-related treatment-emergent adverse events occurring in at least 5% of patients (safety-evaluable patients)
| Event | Ruxolitinib (N = 71) | |
|---|---|---|
| Any grade | Grade 3/4 | |
| Anemia | 25 (35.2) | 20 (28.2) |
| Platelet count decreased* | 23 (32.4) | 21 (29.6) |
| Neutrophil count decreased | 19 (26.8) | 15 (21.1) |
| White blood cell count decreased | 14 (19.7) | 8 (11.3) |
| Thrombocytopenia* | 11 (15.5) | 9 (12.7) |
| Alanine aminotransferase increased | 8 (11.3) | 1 (1.4) |
| Lymphocyte count decreased | 7 (9.9) | 7 (9.9) |
| Peripheral edema | 6 (8.5) | 1 (1.4) |
| Aspartate aminotransferase increased | 4 (5.6) | 0 |
| Dizziness | 4 (5.6) | 0 |
| Fatigue | 4 (5.6) | 1 (1.4) |
| Pneumatosis intestinalis | 4 (5.6) | 4 (5.6) |
| Pyrexia | 4 (5.6) | 1 (1.4) |
| Sepsis | 4 (5.6) | 4 (5.6) |
| Event | Ruxolitinib (N = 71) | |
|---|---|---|
| Any grade | Grade 3/4 | |
| Anemia | 25 (35.2) | 20 (28.2) |
| Platelet count decreased* | 23 (32.4) | 21 (29.6) |
| Neutrophil count decreased | 19 (26.8) | 15 (21.1) |
| White blood cell count decreased | 14 (19.7) | 8 (11.3) |
| Thrombocytopenia* | 11 (15.5) | 9 (12.7) |
| Alanine aminotransferase increased | 8 (11.3) | 1 (1.4) |
| Lymphocyte count decreased | 7 (9.9) | 7 (9.9) |
| Peripheral edema | 6 (8.5) | 1 (1.4) |
| Aspartate aminotransferase increased | 4 (5.6) | 0 |
| Dizziness | 4 (5.6) | 0 |
| Fatigue | 4 (5.6) | 1 (1.4) |
| Pneumatosis intestinalis | 4 (5.6) | 4 (5.6) |
| Pyrexia | 4 (5.6) | 1 (1.4) |
| Sepsis | 4 (5.6) | 4 (5.6) |
Data are presented as n (%). The data cutoff was 2 July 2018. Multiple occurrences of the same adverse event in 1 patient were counted only once per preferred term at the highest grade.
The terms “platelet count decreased” and “thrombocytopenia” were used by investigators when reporting adverse events, and therefore were recorded as separate terms in the safety database.
Discussion
Treatment of steroid-refractory aGVHD after HCT remains a challenge. Various treatment strategies have been tested for steroid-refractory aGVHD8,20-25 ; however, the REACH1 study is the first prospective clinical trial demonstrating a clinically meaningful response using modern aGVHD grading and response assessments.16,17 Patients enrolled in the REACH1 study were heavily exposed to systemic corticosteroids before study initiation, regardless of aGVHD grade at enrollment. Fifty-five percent of patients treated with ruxolitinib had a response at day 28, and those who responded had prolonged OS compared with nonresponders (P < .0001). Patients with grade III/IV aGVHD at enrollment who achieved a CR or VGPR (23%) had a median DOR of 345 days with a 12-month OS probability of 82%, which highlights that patients with advanced steroid-refractory aGVHD who are ruxolitinib responsive can be salvaged effectively. No clinically significant difference was observed across the steroid-refractory criteria subgroups, and responses were observed irrespective of the organ involved.
Rates of NRM for patients with steroid-refractory aGVHD are historically high (73% at 12 months in patients treated with inolimomab or etanercept).7,26 Although early mortality was also prevalent in REACH1, the NRM rate was 53% for all patients at 12 months. Patients who responded at day 28 and maintained their response had a 12-month NRM rate of 28%, whereas patients who did not respond to ruxolitinib had a substantially higher NRM rate (84% at 12 months). NRM was not associated with AEs of ruxolitinib. Most deaths were attributable to infections. The high rates of infection and infection-related mortalities observed in this study were likely driven by immune system dysfunction resulting from corticosteroid exposure before initiation of ruxolitinib treatment. Furthermore, development of GVHD alone increases the risk for infections independent of other variables.
Sixty of 71 patients discontinued ruxolitinib, with physician decision and AEs being the most frequent reasons (n = 20, each). It is likely that proactive management of AEs and increased familiarity with the use of ruxolitinib in this patient population may translate into a decreased incidence of discontinuation. Ruxolitinib has been associated with increased rates of infection in patients with myelofibrosis.27 Standard treatment practices for patients with steroid-refractory aGVHD involve effective antimicrobial, antifungal, anti-CMV, and anti-varicella zoster prophylaxis, as well as CMV reactivation surveillance.8,26 The safety profile observed in this study was consistent with that of patients with steroid-refractory aGVHD and the known AEs of ruxolitinib. The cumulative incidence of CMV events (19.7%; infection, 12.7%; viremia, 5.6%) was comparable to reported CMV reactivation rates in patients with steroid-refractory aGVHD (range, 33.3%-51.2%).13,21,26 The choice of CMV prophylaxis was at the discretion of the treating physician. With the approval of letermovir, use of CMV-specific prophylaxis may limit the risk for CMV reactivation and infection.28 No cases of Epstein-Barr virus-mediated posttransplant lymphoproliferative disorder were observed.
Oral ruxolitinib displayed good absorption even among patients with extensive GI involvement. Pharmacokinetic analyses demonstrated that sex, concomitant use of moderate or potent cytochrome P450 3A4 inhibitors, grade IV aGVHD, and liver involvement were significant predictors of variability in ruxolitinib CL/F. Although available data did not allow for direct conclusions to be drawn between pharmacokinetic parameters and organ involvement, 44.8% of patients with grade III/IV aGVHD and nonskin involvement responded to ruxolitinib treatment in this study, suggesting that GI involvement was not prohibitive of response.
With 55% of patients responding to ruxolitinib by day 28, identification of patients likely to benefit from ruxolitinib is desirable. In a model-based multivariate analysis, aGVHD grade at therapy onset was an independent prognostic factor (P = .0042). Our analyses indicate that increased duration of corticosteroid use before enrollment was significantly associated with reduced OS and increased NRM. Median duration of corticosteroid use in patients with progressive aGVHD after 3 days or aGHVD after 7 days of primary treatment was 14 and 13 days, respectively, suggesting potential opportunity for earlier intervention. As previously observed,20 these findings suggest that patients may benefit from rapid initiation of second-line therapy at the onset of signs of steroid refractoriness and before advanced organ injury or development of severe aGVHD. Examination of response kinetics in patients who responded by day 28 indicates that ruxolitinib, when efficacious, induces early (ie, first response on or before day 14 in 61% of patients) and durable responses.
Baseline levels of ST2 and TNFR1, but not REG3A or Trappin-2/Elafin, were associated with response to treatment in this study. In a prior study of steroid-resistant aGVHD, REG3A levels, when assayed after 1 week of corticosteroid use, were prognostic of 4-week response, 1-year OS, and 1-year NRM.29 In contrast, in our study, REG3A was measured at enrollment into the study, and not at a uniform time after initial onset of corticosteroid use. Another possible explanation for the discrepancy is that ruxolitinib may overcome the negative prognostic value of REG3A. Broad proteomic analysis revealed decreases in IL-17-driven inflammation and corresponding increases in hematopoietic activation after ruxolitinib treatment, suggesting that targeted inhibition of proinflammatory pathways spares growth factors needed for lymphocyte expansion.
Meaningful comparisons are difficult to make across steroid-refractory aGVHD studies as a result of heterogeneous definitions of steroid-refractory disease, small sample sizes, and varying definitions and timing of response assessments. Nonetheless, clinical outcomes observed in REACH1 are encouraging in the context of historical data. The 42.6% 1-year OS rate for all patients receiving ruxolitinib was comparable or favorable to 1-year OS rates among patients treated with vedolizumab (47%),30 antithymocyte globulin (39%),21 brentuximab vedotin (38%),24 or infliximab (∼10%).23 Mesenchymal stem cells have been studied extensively in steroid-refractory aGVHD, with varying response rates.25 However, a recent phase 3 study evaluating mesenchymal stem cells did not meet its primary end point of improved day 28 response rate vs placebo when added to second-line therapy.31 The ongoing REACH2 phase 3 randomized study of ruxolitinib vs best available therapy in patients with steroid-refractory aGVHD (NCT02913261) will further establish the role of JAK inhibitors in the treatment of steroid-refractory aGVHD.
A limitation of this study was the heterogeneous definition of steroid-refractory aGVHD, which was anticipated and accounted for in the eligibility criteria. At the time of this analysis, data were not mature enough to assess long-term outcomes for survival or rates of cGVHD. Furthermore, although patients could receive prophylactic treatment of infections as per institutional standards, detailed data regarding usage were not available; therefore, uniformity of prophylactic regimens across centers cannot be assessed. Finally, the single-group, nonrandomized nature of REACH1 did not allow for comparisons with other available therapeutics.
In summary, findings from REACH1 suggest that ruxolitinib is an effective treatment option for patients with steroid-refractory aGVHD. Responses to ruxolitinib seen at day 28 were durable and were associated with improved survival when compared with survival rates among nonresponders. The safety profile was consistent with expectations for ruxolitinib and patients with steroid-refractory aGVHD.
Presented in abstract form at the 60th annual meeting of the American Society of Hematology, San Diego, CA, 1-4 December 2018 (abstract #601); the 2019 Transplantation & Cellular Therapy Meeting, Houston, TX, 20-24 February 2019 (abstract #66); and the 45th Annual Meeting of the European Society for Blood and Marrow Transplantation, Frankfurt, Germany, 24-27 March 2019 (abstract #OS7-1).
Access to individual patient-level data are not available for this study. For original data requests, please contact skanthala@incyte.com.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
The authors thank the patients, families, and caregivers who participated in this study, as well as the staff at each study site. The authors thank Sherry Owens and Michael Pratta (both of Incyte Corporation) for their assistance with proteomic analysis. Writing assistance was provided by Jane Kovalevich, at Complete Healthcare Communications, LLC (North Wales, PA), a CHC Group company, and was funded by Incyte Corporation.
This study was supported by research funding from Incyte Corporation. M.-A.P. received support, in part, from National Institutes of Health/National Cancer Institute Cancer Center Support Grant P30 CA008748.
Authorship
Contribution: M.J. contributed to study design, data analysis, data interpretation, and manuscript writing; M.-A.P., S.F., F.W.D., and L.C.-S. contributed to data acquisition, data analysis, data interpretation, and manuscript writing; M.A.S. and M.C.A. contributed to study design, data acquisition, data analysis, data interpretation, and manuscript writing; H.A. contributed to data acquisition, data interpretation, and manuscript writing; N.N.S. contributed to data acquisition and manuscript writing; Y.-B.C. contributed to study design, data acquisition, and manuscript writing; C.T. contributed to study design, statistical analysis, data interpretation, and manuscript writing; M.D.H. contributed to study design, data acquisition, and data interpretation related to the biomarker analyses and manuscript writing; H.J.K. contributed to study design; and all authors, with the exception of H.J.K. (deceased), read and approved the final version of the manuscript for publication.
Conflict-of-interest disclosure: M.J. reports receiving consulting fees from Incyte Corporation, Kadmon, and Genentech and receiving institutional research support from Mallinckrodt and Janssen. M.-A.P. reports receiving institutional research support for clinical trials from Incyte Corporation; honoraria from AbbVie, Bellicum, Bristol-Myers Squibb, Incyte Corporation, Merck, Novartis, Nektar Therapeutics, and Takeda; serving on data and safety monitoring boards for Servier and Medigene; and serving on scientific advisory boards for MolMed and NexImmune. M.A.S. reports receiving personal fees and research grant support from Incyte Corporation, Amgen, AbbVie, Astellas, Pfizer, Sanofi/Genzyme, Takeda, and Merck; receiving personal fees from Partners Therapeutics, FlatIron, and NovoNordisk; and receiving research grant support from Seattle Genetics, PBD Inc, Genentech, Cellect, Fortis Therapeutics, Bristol-Myers Squibb, and Celgene. H.A. reports receiving consulting fees from Incyte Corporation. N.N.S. reports receiving consulting fees from Incyte Corporation; serving on scientific advisory boards for Kite, Juno, and Cellectar; and receiving institutional research support for clinical trials from Miltenyi Biotec. Y.-B.C. reports receiving consulting fees from Incyte Corporation, Takeda, Magenta, and Kiadis and serving on data and safety monitoring boards for Actinium, Equillium, and AbbVie; S.F. reports receiving personal fees and other support for serving on advisory boards and speakers’ bureaus for Amgen, Incyte Corporation, Jazz Pharmaceuticals, Gilead, GlaxoSmithKline, Novartis, Bristol-Myers Squibb, and Pfizer; and receiving personal fees and other support for serving on a speakers’ bureau for Stemline Pharmaceuticals, Janssen Pharmaceuticals, Takeda Pharmaceuticals, and Karyopharm. F.W.D., M.C.A., and C.T. report employment by and stock ownership in Incyte Corporation. M.D.H. reports employment by and stock ownership in Incyte Corporation and has a patent pending for Biomarkers for Graft Versus Host Disease. H.J.K. served on an advisory board and received research funding from Incyte Corporation. L.C.-S. declares no competing financial interests.
H. Jean Khoury died on 22 May 2017.
A complete list of REACH1 investigators appears in the supplemental Appendix.
Correspondence: Madan Jagasia, Vanderbilt-Ingram Cancer Center, 1301 Medical Center Dr #1710, Nashville, TN 37232; e-mail: madan.jagasia@vanderbilt.edu.
