

Background:
A key component of COG maintenance chemotherapy for pediatric B-ALL has been the inclusion of vincristine/steroid pulses administered every 4 weeks. With the intensification of pre-maintenance therapy and modern risk stratification, there is uncertainty regarding the optimal frequency of these pulses in the context of modern ALL therapy. AALL0932 was designed to optimize maintenance therapy by asking two questions: (1) whether giving vincristine/dexamethasone (VCR/DEX) pulses every 12 weeks was non-inferior to every 4 week pulses; and (2) whether a starting weekly oral methotrexate (MTX dose) of 40 mg/m²/dose would be superior to the standard 20 mg/m2/dose. We previously reported that there was no benefit to intensifying oral methotrexate during maintenance therapy (ASH 2017). We now report on the outcomes of the VCR/DEX pulses.
Methods:
Average risk (AR) patients participating in the randomization had NCI SR B-ALL without CNS3 or testicular leukemia, unfavorable genetic characteristics or Down syndrome, AND either favorable genetics (trisomies of chromosomes 4 &10 or ETV6/RUNX1 fusion) with Day 8 peripheral blood (PB) minimal residual disease (MRD) ≥ 0.01% or CNS2 status, Day 29 bone marrow (BM) MRD < 0.01%, OR if neutral cytogenetics, had Day 8 PB MRD < 1% and Day 29 BM MRD < 0.01%. AR patients were randomized to 1 of 4 Maintenance regimens using a 2 x 2 factorial design: (A): VCR/DEX pulses every 4 weeks and oral MTX 20 mg/m²/week (standard arm); (B): VCR/DEX pulses every 4 weeks and oral MTX 40 mg/m²/week; (C): VCR/DEX pulses every 12 weeks and oral MTX 20 mg/m²/week; and (D): VCR/DEX pulses every 12 weeks and oral MTX 40 mg/m²/week. Results from the MTX randomization have been previously reported (ASH 2017).
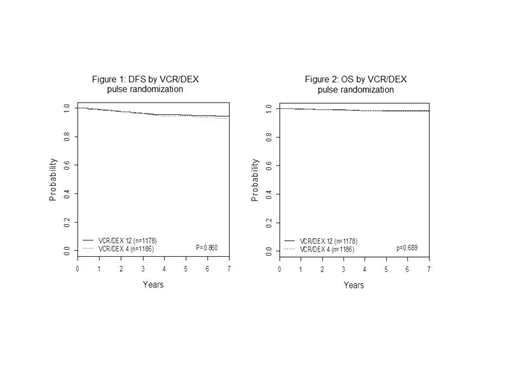
Between 2010 and 2016, 2364 patients were randomized at the start of maintenance to VCR/DEX pulses every 4 weeks [Arms A and B (n=1186)] or VCR/DEX pulses every 12 weeks [Arms C & D (n=1178)].
Results:
The 5-year disease-free survival (DFS) (±SE) measured from the time of randomization for the AR subset of patients randomized to receive VCR/DEX pulse every 4 weeks vs. every 12 weeks was 94.1% ±1.0% vs. 95.1% ±0.9%, respectively (one-sided p=0.86 indicating no evidence of DFS inferiority for 12 week frequency). The 5-year overall survival (OS) (±SE) for the AR patients randomized to receive VCR/DEX pulse every 4 weeks vs. every 12 weeks was 98.3% ±0.5%, vs. 98.6% ±0.5%, respectively (one sided p=0.69). There was no evidence of significant interaction between the MTX and VCR/DEX pulses randomizations.
Conclusions:
AALL0932 demonstrated that the AR subset of patients with SR B-ALL who received VCR/DEX pulses every 12 weeks maintained outstanding outcomes similar to those who received pulses every 4 weeks. The decreased frequency of VCR/DEX pulses will be incorporated into frontline B-lineage COG ALL trials thereby dramatically improving patient and family quality of life.
Angiolillo:Servier Pharmaceuticals: Consultancy. Schore:Janssen Research & Development, LLC: Research Funding; AMGEN INC: Research Funding. Zweidler-McKay:ImmunoGen: Employment. Borowitz:Beckman Coulter: Honoraria. Relling:Servier Pharmaceuticals: Research Funding. Raetz:Pfizer: Research Funding. Loh:Medisix Therapeutics, Inc.: Membership on an entity's Board of Directors or advisory committees. Hunger:Bristol Myers Squibb: Consultancy; Amgen: Consultancy, Equity Ownership; Jazz: Honoraria; Novartis: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal