


Background: Quizartinib, a once-daily, oral, highly potent and selective FLT3 inhibitor, demonstrated a significant improvement in survival vs SC in FLT3-ITD-positive R/R AML in the global, randomized, phase 3 QuANTUM-R study (Cortes et al. Lancet Oncol, 2019; NCT02039726). Patients with R/R FLT3-ITD-positive AML were randomized 2:1 to receive single agent quizartinib or investigator's choice of pre-selected SC. We investigated the effects of baseline co-mutations and FLT3-ITD VAF on overall survival (OS) and response (composite complete remission [CRc]) to quizartinib and SC in QuANTUM-R.
Methods: We analyzed 37 recurrently mutated genes in AML in baseline bone marrow samples from 304 patients (82.8% of ITT population [N = 367; quizartinib, n = 245; SC, n = 122]) with R/R FLT3-ITD-positive AML using next-generation sequencing and a customized Archer® Core Myeloid panel. Positive mutation status was defined as ≥ 1 mutation detected in the gene region using a VAF cutoff of 2.7%. FLT3-ITD VAF was measured separately by the Navigate BioPharma FLT3 Mutation Assay (polymerase chain reaction-based, VAF cutoff of 3%). Low and high FLT3-ITD VAF were defined as ≤25% and >25%, respectively.
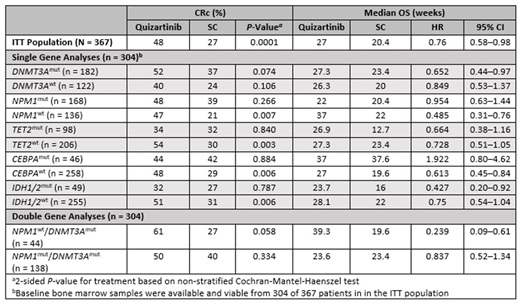
Results: In addition to FLT3-ITD, 5 key co-mutations were detected: DNMT3Amut (n = 182/304 [59.9%]), NPM1mut (n = 168/304 [55.3%]), TET2mut (n = 98/304 [32.2%]), IDH1/2mut (n = 49/304 [16.1%]) and CEBPAmut (n = 46/304 [15.1%]). Median OS was numerically longer with quizartinib vs SC in patients with DNMT3Amut, TET2mut, IDH1/2mut and NPM1mut, but not CEBPAmut (Table). CRc rates were numerically higher with quizartinib vs SC for each of the 5 key baseline co-mutations. For single gene mutations, the longest median OS was seen in patients with CEBPAmut treated with quizartinib or SC (37 and 37.6 weeks, respectively). As the majority of NPM1mut patients were also DNMT3Amut (138/168, 82%), we examined various permutations of these two mutations. Patients with NPM1wt/DNMT3Amut had significantly longer median OS with quizartinib vs SC (39.3 vs 19.6 weeks, respectively; HR, 0.239; P = 0.003 [Table]) while NPM1mut/DNMT3Amut patients had lower and similar median OS between the 2 arms (23.6 vs 23.4 weeks, respectively). Quizartinib treatment showed significantly longer median OS vs SC in patients with high FLT3-ITD VAF (23.9 vs 17 weeks respectively; HR, 0.689, P = 0.0148), while the median OS in patients with low FLT3-ITD VAF was similar (34.1 vs 26.6 weeks, respectively; HR, 0.857, P = 0.535).
Conclusions: This is the first evaluation of the effect of baseline co-mutations on clinical outcomes in a large trial of R/R AML patients with FLT3-ITD mutations treated with quizartinib. Key co-mutations identified in this analysis were found to potentially impact treatment response and OS with quizartinib, relative to SC. Despite relatively low CRc rates in patients with IDH1/2mut, this group-as well as those with NPM1wt-derived the greatest OS benefit from quizartinib compared with SC on QuANTUM-R. CEBPA mutations were associated with high CRc rates and relatively long median OS, regardless of treatment arm. Patients with NPM1mut had a higher CRc rate with quizartinib vs SC, but this did not translate into longer survival on either arm compared with NPM1wt. A high allelic burden of FLT3-ITD at the time of salvage therapy was associated with relatively poorer median OS; quizartinib significantly improved survival of patients with high FLT3-ITD VAF relative to SC. Although these results require confirmation in an independent dataset, the modulatory effects of baseline co-mutations on treatment response and OS with quizartinib appear to differ from other FLT3 inhibitors. Our results indicate that a subset of R/R AML patients may particularly derive clinical benefit from quizartinib.
Perl:Daiichi Sankyo: Consultancy, Honoraria, Other, Research Funding; Arog: Consultancy, Other: Non-financial support included travel costs for advisory board meetings.; AbbVie: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.; Actinium Pharmaceuticals: Consultancy, Honoraria, Other: Clinical Advisory Board member, Research Funding; Agios: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Non-financial support included travel costs for advisory board meetings.; Jazz: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.; NewLink Genetics: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.; Takeda: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.; Bayer: Research Funding; BioMed Valley Discoveries: Research Funding; FujiFilm: Research Funding; Novartis: Honoraria, Other: Advisory board, Non-financial support included travel costs for advisory board meetings as well as a medical writing company that assisted with manuscript preparation/submission and slide deck assembly for academic meeting presentations of the data., Research Funding; Astellas: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings as well as a medical writing company that assisted with manuscript preparation/submission and slide deck assembly for academic meeting presentations of trial data., Research Funding. Cortes:Astellas Pharma: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Merus: Consultancy, Honoraria, Research Funding; Forma Therapeutics: Consultancy, Honoraria, Research Funding; Biopath Holdings: Consultancy, Honoraria; BiolineRx: Consultancy; Pfizer: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Daiichi Sankyo: Consultancy, Honoraria, Research Funding; Bristol-Myers Squibb: Consultancy, Research Funding; Sun Pharma: Research Funding; Immunogen: Consultancy, Honoraria, Research Funding. Ganguly:Kite Pharma: Honoraria, Other: Advisory Board; Janssen: Honoraria, Other: Advisory Board; Seattle Genetics: Speakers Bureau; Daiichi Sankyo: Research Funding. Khaled:Omeros: Consultancy; Alexion: Consultancy, Speakers Bureau; Daiichi Sankyo: Other: Travel support. Krämer:Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Daiichi-Sankyo: Honoraria, Membership on an entity's Board of Directors or advisory committees; Bayer: Research Funding; BMS: Research Funding. Martinelli:Novartis: Consultancy, Other: trial grant; Roche: Consultancy, Other: trial grant; Janssen: Consultancy, Other: trial grant; Incyte: Consultancy, Other: trial grant; Pfizer: Consultancy, Other: trial grant; Amgen: Consultancy, Other: trial grant; Celgene: Consultancy, Honoraria, Other: trial grant; Ariad: Consultancy, Other: trial grant; Abbvie: Consultancy, Honoraria, Other: trial grant; Daiichi Sankyo: Consultancy, Honoraria. Russell:Pfizer Inc: Consultancy, Honoraria, Speakers Bureau; Astellas: Consultancy, Honoraria, Speakers Bureau; Jazz: Consultancy, Honoraria, Speakers Bureau; DSI: Consultancy, Honoraria, Speakers Bureau. Chang:Daiichi Sankyo: Employment. Mires:Daiichi Sankyo: Employment. Kato:Daiichi Sankyo, Inc.: Employment; Celgene: Employment, Equity Ownership. Zhang:Daiichi Sankyo: Employment. Korkhov:Precision for Medicine, Inc.: Employment; Daiichi Sankyo: Consultancy. Wang:Precision for Medicine, Inc.: Employment; Daiichi Sankyo: Consultancy. Günnel:Precision for Medicine, Inc.: Employment; Daiichi Sankyo: Consultancy. Sumi:Daiichi Sankyo, Inc.: Employment. Isoyama:Daiichi Sankyo Co, Ltd: Employment. Lesegretain:Daiichi-Sankyo Inc.: Employment, Equity Ownership. Berisha:Daiichi Sankyo: Employment. Dos Santos:Daiichi Sankyo: Employment. Levis:Agios: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Novartis: Consultancy, Research Funding; FUJIFILM: Consultancy, Research Funding; Menarini: Consultancy, Honoraria; Astellas: Consultancy, Research Funding; Daiichi Sankyo Inc: Consultancy, Honoraria.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal