


Introduction: In the phase 3 QuANTUM-R trial, once-daily, oral, highly potent and selective FLT3 inhibitor Q improved clinical benefits vs SC (median overall survival [mOS], 6.2 vs 4.7 mo [HR, 0.76 (95% CI, 0.58-0.98); P = .02]; composite complete remission [CRc], 48% vs 27%; median duration of CRc, 12.1 vs 5.0 wk) in 367 pts with R/R FLT3-ITD AML (Cortes et al. Lancet Oncol, 2019; NCT02039726). Prior to randomization, 25% (Q) and 23% (SC) of pts had 1 prior HSCT. An OS sensitivity analysis, with censoring at the time of any subsequent HSCT during QuANTUM-R, was supportive (mOS, 5.7 vs 4.6 mo [HR, 0.79 (95% CI, 0.59-1.05)]; P = .05). Post hoc analyses of characteristics and clinical outcomes in pts who underwent subsequent HSCT in QuANTUM-R are reported.
Methods: Pts aged ≥ 18 y with FLT3-ITD R/R AML receiving Q (60 mg [30-mg lead-in]) or 1 of 3 prespecified high- or low-intensity SC regimens and underwent subsequent HSCT as part of the open-label, randomized QuANTUM-R trial were analyzed. Pts receiving HSCT in the Q arm could resume maintenance Q 30-100 days after HSCT. Decisions to proceed to HSCT and resume Q after HSCT were made per investigator discretion/institutional policies.
Results: Of 367 randomized pts, 85 in the Q arm underwent any subsequent HSCT (allogenic HSCT [allo-HSCT], 84 [6 with and 78 w/o additional AML therapy]; autologous HSCT, 1) and 19 in the SC arm underwent any HSCT (5 with and 14 w/o additional AML therapy]). Median age (range) was lower in pts with any HSCT (Q, 49 [19-71] y; SC, 44 [23-67] y) vs pts w/o (Q, 58 [19-81] y; SC, 59 [18-78] y).
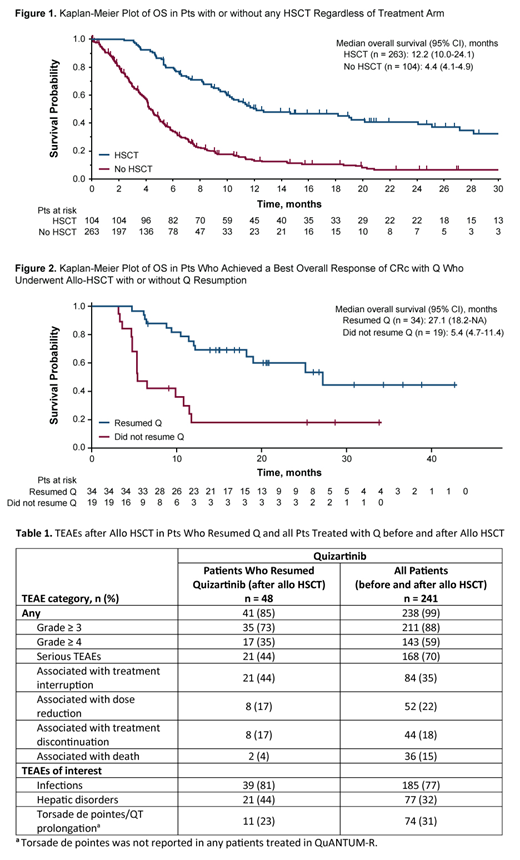
Q + SC pooled data showed a longer mOS (95% CI) in 104 pts with any HSCT vs 263 w/o (12.2 [10.0-24.1] vs 4.4 [4.1-4.9] mo; P < .0001; Fig 1); 1-year OS probabilities (95% CI) were 50% (40%-60%) vs 13% (9%-18%). Among pts preselected for high-intensity therapy (Q [n = 188] + SC [n = 93]), mOS in the pooled high-intensity group was 11.9 (10.0-24.0) mo with any HSCT vs 4.6 (4.1-5.4) mo w/o. Among pts preselected for low-intensity therapy, 13/57 in the Q arm and 0/29 in the SC arm underwent any HSCT; mOS in the pooled low-intensity group was 32.4 (6.2-NA) mo with any HSCT vs 4.1 (2.7-4.6) mo w/o.
In pts with CRc (last recorded response prior to allo-HSCT), mean time (range) to allo-HSCT was 13.3 (5.9-26.9) wk with Q and 12.1 (6.3-28.6) wk with SC. Q + SC pooled data showed that mOS (95% CI) was longer in pts with a CRc prior to allo-HSCT vs pts w/o CRc (20.1 [11.7-NA] vs 8.8 [7.0-11.4] mo).
Survival outcomes by treatment were similar regardless of study treatment, with longer mOS in pts with any HSCT vs pts w/o (Q, 11.9 [10.2-25.1] vs 4.5 [4.1-5.4] mo; SC, 12.7 [6.1-NA] vs 4.0 [2.7-5.0] mo); respective 1-year OS probabilities (95% CI) were 50% (39%-60%) vs 13% (8%-20%) and 51% (26%-70%) vs 12% (6%-21%). In the Q arm, mOS (95% CI) was longer in pts with a best response of CRc who resumed Q after allo-HSCT (27.1 [18.2-NA] mo) vs pts not resuming Q (5.4 [4.7-11.4] mo; Fig 2).
In 48 pts (62%) in the Q arm resuming Q after allo-HSCT, median time (range) from allo-HSCT to Q resumption was 65 (30-106) d. Four pts (5%) in the Q arm died < 30 days after allo-HSCT. As of 2/22/2018, 46 of 78 pts in the Q arm (59%) and 9 of 14 pts in the SC arm (64%) with allo-HSCT w/o additional AML therapy died, primarily due to AML disease progression (Q, 31 [40%]; SC, 7 [50%]). The frequency of treatment-emergent adverse events (TEAEs) was mostly lower in pts resuming Q after allo-HSCT than in the overall Q population (Table 1); TEAEs of interest were similar. Long-term survivor data will be presented.
Conclusions: Independent of HSCT, Q improved survival vs SC in pts with FLT3-ITD R/R AML in QuANTUM-R. Q + SC pooled analyses showed longer survival in pts with HSCT vs pts w/o and in pts with CRc prior to allo-HSCT. Importantly, survival post-HSCT was similar in the Q and SC arms, indicating that pts eligible for HSCT were appropriately transplanted, and the higher HSCT rate in the Q arm was beneficial to pts. More pts treated with Q underwent HSCT, likely due to a higher rate and duration of CRc with Q vs SC and better overall fitness. In pts preselected for low-intensity SC at study entry, 13 were able to undergo HSCT after Q treatment. Resumption of Q after HSCT was associated with better survival outcomes and was tolerable. These data illustrate the value of using Q to target the FLT3-ITD mutation as a part of the overall treatment sequence in pts with FLT3-ITD R/R AML.
Ganguly:Seattle Genetics: Speakers Bureau; Janssen: Honoraria, Other: Advisory Board; Kite Pharma: Honoraria, Other: Advisory Board; Daiichi Sankyo: Research Funding. Cortes:Bristol-Myers Squibb: Consultancy, Research Funding; BiolineRx: Consultancy; Daiichi Sankyo: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Astellas Pharma: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Sun Pharma: Research Funding; Immunogen: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Research Funding; Novartis: Consultancy, Honoraria, Research Funding; Forma Therapeutics: Consultancy, Honoraria, Research Funding; Biopath Holdings: Consultancy, Honoraria; Merus: Consultancy, Honoraria, Research Funding. Krämer:Daiichi-Sankyo: Honoraria, Membership on an entity's Board of Directors or advisory committees; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; BMS: Research Funding; Bayer: Research Funding. Levis:Amgen: Consultancy, Honoraria; Agios: Consultancy, Honoraria; Daiichi Sankyo Inc: Consultancy, Honoraria; Astellas: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Menarini: Consultancy, Honoraria; FUJIFILM: Consultancy, Research Funding. Martinelli:Daiichi Sankyo: Consultancy, Honoraria; Pfizer: Consultancy, Other: trial grant; Celgene: Consultancy, Honoraria, Other: trial grant; Janssen: Consultancy, Other: trial grant; Incyte: Consultancy, Other: trial grant; Amgen: Consultancy, Other: trial grant; Abbvie: Consultancy, Honoraria, Other: trial grant; Novartis: Consultancy, Other: trial grant; Roche: Consultancy, Other: trial grant; Ariad: Consultancy, Other: trial grant. Perl:Novartis: Honoraria, Other: Advisory board, Non-financial support included travel costs for advisory board meetings as well as a medical writing company that assisted with manuscript preparation/submission and slide deck assembly for academic meeting presentations of the data., Research Funding; Bayer: Research Funding; BioMed Valley Discoveries: Research Funding; FujiFilm: Research Funding; Takeda: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.; Astellas: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings as well as a medical writing company that assisted with manuscript preparation/submission and slide deck assembly for academic meeting presentations of trial data., Research Funding; Daiichi Sankyo: Consultancy, Honoraria, Other, Research Funding; Arog: Consultancy, Other: Non-financial support included travel costs for advisory board meetings.; AbbVie: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.; Actinium Pharmaceuticals: Consultancy, Honoraria, Other: Clinical Advisory Board member, Research Funding; Agios: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Non-financial support included travel costs for advisory board meetings.; Jazz: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.; NewLink Genetics: Consultancy, Honoraria, Other: Non-financial support included travel costs for advisory board meetings.. Russell:Astellas: Consultancy, Honoraria, Speakers Bureau; Pfizer Inc: Consultancy, Honoraria, Speakers Bureau; Jazz: Consultancy, Honoraria, Speakers Bureau; DSI: Consultancy, Honoraria, Speakers Bureau. Arunachalam:Daiichi Sankyo: Employment. Gammon:Daiichi Sankyo: Consultancy. Lesegretain:Daiichi-Sankyo Inc.: Employment, Equity Ownership. Mires:Daiichi Sankyo: Employment. Namuyinga:Daiichi Sankyo: Employment. Zhang:Daiichi Sankyo: Employment. Khaled:Omeros: Consultancy; Daiichi Sankyo: Other: Travel support; Alexion: Consultancy, Speakers Bureau.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal