

Background
Multiparametric flow cytometry (MFC) is critical in the diagnosis and management of pediatric acute lymphoblastic leukemia (ALL), through immunophenotyping (IP), and minimal residual disease (MFC MRD) analysis.
The aberrant expression of myeloid markers in B- and T-lineage ALL is a well-known phenomenon. It may be the result of an adaptive mechanism by lineage switch (SW), defined as any variation of blast IP over time.
CD371 is a transmembrane glycoprotein usually expressed on normal myeloid cells and most of the myeloid blasts. Aberrant expression of CD371 was observed in DUX4-rearranged B cell precursor ALL (BCP ALL).
Aims
To investigate the clinical and biological features of CD371 positive (CD371+) pediatric BCP ALL, pointing out its potential implication in MFC MRD monitoring on Day 15.
Materials and Methods
From June 2014 to January 2017, 862 children with newly diagnosed t(9;22)(q34.1;11.2);BCR-ABL1 negative BCP ALL, were consecutively enrolled in the AIEOP BFM ALL 2009 study by AIEOP centers. Peripheral blood (PB) and bone marrow (BM) samples (SMPs) were processed and analyzed in the Laboratory of Diagnosis and Research of Pediatric Hematology-Oncology, University of Padua, Italy, according to standardized operating protocols designed by the AIEOP BFM Flow Network. At diagnosis, 9 combinations of 8 monoclonal antibodies (MoAbs) were used for IP. MFC MRD (Day 8 on PB, Day 15, 33, and 78 on BM) was performed with 2 combinations of 8 MoAbs from June 2014 to May 2016. Later, a dry 10 colors preformulated tube was adopted for MFC MRD monitoring.
Results
At diagnosis, CD371 expression was assessed in 823 of 862 (95.5%) SMPs by as many patients (pts; age: 1-17 years; male/female: 446/377). Of those, CD371 was positive in 75 of 823 SMPs (9.1%). CD371 positivity was associated with older age, euploidy, a more immature immunophenotype (B-I as per EGIL classification), and the aberrant expression of CD2 antigen, as well as at least one myeloid marker (Table). CD371+ SMPs showed a stronger expression of CD34, CD45, and CD58 antigens than CD371 negative SMPs (Table).
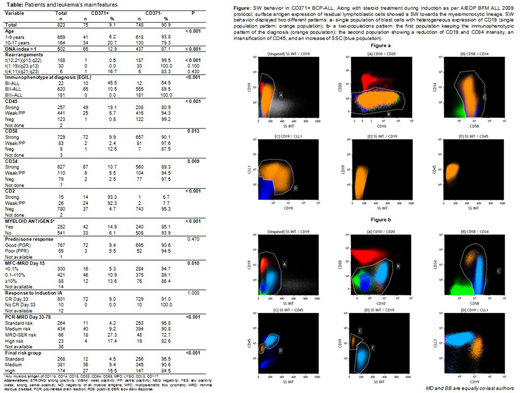
We performed MFC MRD analysis on 207 SMPs of CD371+ BCP ALL (42 on Day 8, 72 on Day 15, 40 on Day 33, and 53 on Day 78). During the first 15 days of Induction therapy, a monocytoid population appeared in 76 SMPs [26 of 42 (61.9%) on Day 8 and 50 of 72 (69.4%) on Day 15]. It was characterized by a strong expression of CD34, CD58 and CD45, reduced expression of CD19, and high SSC. We interpreted that phenomenon as an SW to the myelomonocytic lineage, as previously described in a subtype of BCP ALL expressing CD2 at diagnosis. Myelomonocytic SW displayed 2 different patterns: (a) a single population of blasts with heterogeneous expression of CD19 (strong to dim/negative); (b) 2 distinct populations: the first one with the IP of diagnosis, the second one showing a downregulation of CD19 and CD34, an intensification of CD45, and an increase of SSC (Figure). At the same time points, a clear monocytoid population was visible on May-Grunwald-Giemsa stained smears. The comparison between MFC MRD and PCR MRD data showed a higher concordance when both the populations were included in the final amount of blasts on Day 15 (concordance rate: 89% vs. 82%). SW was transient and disappeared after Day 15, even though chemotherapy was always carried on as per therapeutic ALL protocol. CD371 antigen was an accurate marker of SW in our cohort [sensitivity = 0.93 (95% CI ± 0.06), specificity = 0.98 (95% CI ± 0.005), accuracy = 0.98].
Finally, CD371 positivity was associated with a worse response to Induction therapy, showing a higher proportion of pts enrolled in the high therapeutic risk group of the trial, most frequently due to a slow early response according to PCR MRD on Day 33 and 78 (Table).
Conclusions
We described a new subtype of pediatric BCP ALL, characterized by the aberrant expression of CD371 and a potential myelomonocytic SW during the first phase of Induction Therapy. Accurate identification of the lineage SW is mandatory to properly assess MFC MRD on Day 15 in these pts, avoiding an underestimation of blast cells. This is particularly important, considering that CD371+ BCP ALL was associated with a poor response to Induction therapy. Even in presence of a prevalent monocytoid population, chemotherapy should be carried on according to a therapeutic protocol for ALL. CD371 antigen should be part of IP diagnosis panel for ALL. A multicenter study of AIEOP BFM Flow Network centers is ongoing.
Brüggemann:Amgen: Membership on an entity's Board of Directors or advisory committees; Incyte: Membership on an entity's Board of Directors or advisory committees; Roche: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal