


Clonal hematopoiesis associated with loss of HLA class I alleles due to somatic mutations and/or 6p loss of heterozygosity (LOH) is frequent in immune aplastic anemia (AA). HLA-B*40:02 is more likely to be involved in HLA loss in Japanese AA patients, suggesting a role for this allele in immune pathophysiology (Zaimoku Y et al, Blood 2017). Mutations in non-B*40:02 HLA class I alleles have been reported in a limited number of patients from the United States (Babushok D et al, Blood Adv 2017) and Japan (Mizumaki H et al, 60th ASH meeting), but their prevalence and clinical significance are not well characterized. We investigated somatic mutations of HLA class I alleles, HLA allele frequencies, and their correlations with outcomes of therapy in a total of 532 AA patients, aged 2 years or older, treated on various Hematology Branch protocols (clinicaltrials.gov NCTs 00001964, 00061360, 00195624, 00260689, 00944749, 01193283, and 01623167).
HLA allele-lacking (HLA-) monocytes from cryopreserved peripheral blood mononuclear cells were screened by flow cytometry after staining with allele-specific monoclonal antibodies for HLA-A and/or HLA-B (HLA-flow) in 172 AA patients. HLA- monocytes accounting for 0.5% to 100% (median 9.5%) of total monocytes were detected in 49 (28%) of the 172 patients and in 59 (15%) of 382 alleles analyzed (Figure 1). Loss of cell surface expression was frequent for HLA-B14 (46%), B27 (33%), B49 (33%), A68 (26%), A2 (23%), B40 (21%), and B8 (21%). One percent to 60% (median, 8.9%) of glycosylphosphatidylinositol-linked protein-negative (GPI-) monocytes were also present in 43% (21 of 49) of the patients with HLA- monocytes, but GPI- clones had normal HLA cell surface expression.
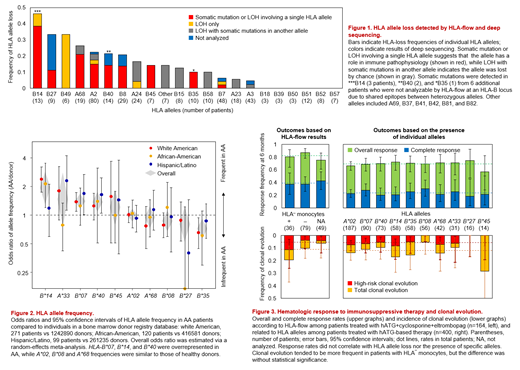
Deep sequencing of HLA-A, HLA-B and HLA-C on sorted HLA- and HLA+GPI+ monocytes was performed in 42 of the 48 patients from whom adequate cells were available. Somatic mutations and/or LOH corresponding to the lacking alleles were detected in all 42 cases (Figure 1): 9 had both somatic mutations and LOH, 20 had somatic mutations only, and 13 had LOH only. Among the 13 patients who showed only LOH in the absent allele, 6 had somatic mutations in other alleles of HLA+ monocytes that was not analyzable of HLA expression, and 2 had a breakpoint of LOH between HLA-A and HLA-C, leading to loss of a single HLA-A allele. Somatic mutations or LOH involving only one allele were present in 37 patients among 6 HLA-A alleles (in 02:01 [7 patients], 02:05 [1], 02:06 [3], 02:11 [1], 68:01 [2], 68:02 [2]) and 10 HLA-B alleles (07:02 [1], 08:01 [4], 14:01 [1], 14:02 [7], 27:05 [1], 35:02 [1], 35:05 [1], 40:01 [1], 40:02 [3], 45:01 [1]), but were not found in HLA-C alleles.
HLA allele frequencies in AA patients, including 271 white Americans, 120 African-Americans, and 99 Hispanics and Latinos, were compared with ethnicity-matched individuals in bone marrow donor datasets of the National Marrow Donor Program, and underwent random-effects meta-analyses. HLA-B*07, B*14, and B*40 were overrepresented in AA, while A*02, A*68, and B*08 frequencies were similar to those of healthy donors (Figure 2).
In 164 severe AA patients who were initially treated with horse antithymocyte globulin (hATG), cyclosporine, and eltrombopag between 2012 and 2018, 36 and 79 were positive and negative for HLA- monocytes, respectively, and 49 were not tested by HLA-flow. There was no significant difference in overall and complete response rates at six months among the three groups (Figure 3). Clonal evolution, defined as acquisition of abnormal bone marrow cytogenetics or morphology, especially high-risk evolution to chromosome 7 abnormalities, complex cytogenetics, or morphological MDS/AML, tended to be more frequent in patients with HLA- monocytes, compared to the other two groups, but the difference did not reach statistical significance. Clinical outcomes were also assessed according to the presence of specific HLA alleles in 400 severe AA patients who were treated with hATG-based initial immunosuppressive therapy from 2000 to 2018: there was no significant differences in probabilities of response and clonal evolution according to the alleles associated with somatic mutations.
Our study revealed that somatic mutations in HLA genes in AA are broadly distributed, but some alleles are preferentially affected. Inconsistent with previous studies, we found that outcomes of therapy did not significantly correlate with HLA gene mutations or with distinct HLA alleles.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal