

Abstract
Chronic lymphocytic leukemia (CLL) therapy has changed dramatically with the introduction of several targeted therapeutics. Ibrutinib was the first approved for use in 2014 and now is used for initial and salvage therapy of CLL patients. With its widespread use in clinical practice, ibrutinib’s common and uncommon adverse events reported less frequently in earlier clinical trials have been experienced more frequently in real-world practice. In particular, atrial fibrillation, bleeding, infections, and arthralgias have been reported. The management of ibrutinib’s adverse events often cannot be generalized but must be individualized to the patient and their long-term risk of additional complications. When ibrutinib was initially developed, there were limited therapeutic alternatives for CLL, which often resulted in treating through the adverse events. At the present time, there are several effective alternative agents available, so transition to an alternative CLL directed therapy may be considered. Given the continued expansion of ibrutinib across many therapeutic areas, investigation of the pathogenesis of adverse events with this agent and also clinical trials examining therapeutic approaches for complications arising during therapy are needed. Herein, we provide strategies we use in real-world CLL clinical practice to address common adverse events associated with ibrutinib.
Introduction
For patients with chronic lymphocytic leukemia (CLL), the treatment paradigm has shifted from nonspecific chemoimmunotherapy regimens to targeted kinase inhibitors with the goals of maximizing efficacy and minimizing toxicity. Ibrutinib, an oral inhibitor of Bruton tyrosine kinase (BTK), has been at the forefront of the paradigm shift. Inhibition of BTK with ibrutinib blocks many functionalities in the B-cell receptor signaling pathway that are crucial for differentiation, migration, signaling, proliferation, and survival of the malignant CLL B-lymphocytes.1-3 Pivotal phase 2 and 3 clinical trials (RESONATE and RESONATE2) demonstrated prolonged survival for ibrutinib-treated CLL patients in both the frontline and relapsed setting when compared with standard-of-care therapies.4-6 As such, ibrutinib was approved for marketing in 2014 and has been rapidly adopted as an efficacious therapeutic option for all patients with CLL.
Unfortunately, ibrutinib does not cure CLL, and its efficacy is dependent upon chronic BTK inhibition. At present, ibrutinib is thought to require indefinite administration to ensure continued clinical benefit. With publication of long-term follow-up of the initial studies, it has become apparent that up to 51% of CLL patients have discontinued ibrutinib therapy.7-9 Similarly, a retrospective study of ibrutinib-treated patients in a “real world” setting reported a 41% discontinuation rate.10 Of the patients who discontinued ibrutinib therapy, up to 51% of these discontinuations were secondary to toxicity.10 Therefore, clinicians are left with the dilemma of how to manage patients with ibrutinib intolerance and its complications. In this article, we will review cases of ibrutinib intolerance, report frequency and proposed mechanisms, and discuss our recommended management of these patients. As ibrutinib has only been approved for marketing since 2014 in CLL, these strategies will likely change as more experience is obtained with this agent.
Case 1: atrial fibrillation
The patient, a 76-year-old male with CLL and a history of hypertension and coronary artery disease with 3 prior treatments for CLL, was started on ibrutinib 420 mg by mouth daily 7 months ago secondary to symptomatic splenomegaly. The patient’s CLL-related symptoms resolved within a month of starting ibrutinib therapy. Two weeks ago, he presented to an outside emergency room for evaluation of dyspnea on exertion. Physical examination revealed a rapid, irregular heart rate. An electrocardiogram confirmed atrial fibrillation. The patient was started on rate control with metoprolol and warfarin to prevent thromboembolic events. Yesterday, he presented to the emergency room with severe right-sided low back pain. Abdominal scans revealed a large retroperitoneal bleed.
Frequency of atrial fibrillation
A review of patients treated with ibrutinib in clinical trials and in clinical practice reveals an increased rate of atrial fibrillation from 4% to 10% over what is expected in the general population (1% to 2%; patients >65 years) and cancer patients (4%; Table 1).4-6,10-18 Although CLL patients reportedly have a high prevalence (6%) and incidence (6%) of atrial fibrillation, phase 3 studies of patients receiving ibrutinib vs comparator demonstrate a higher risk of atrial fibrillation in patients who received ibrutinib (Table 1).19 In the phase 3 RESONATE trial, where 195 relapsed or refractory CLL patients were randomized to ibrutinib vs ofatumumab, atrial fibrillation occurred more frequently in the ibrutinib group (5% vs 1%, all grades; 3% vs 0%, grade ≥3).4 With extended follow-up of 19 months, 7% and 4% of ibrutinib-treated patients had developed any grade or grade ≥3 atrial fibrillation, respectively.16,17 It is notable that the incidence of atrial fibrillation decreased over time with no cases reported after 18 months of follow-up (n = 136).17 In the phase 3 RESONATE2 study 135 previously untreated patients were randomized to ibrutinib vs chlorambucil, atrial fibrillation occurred more frequently in the ibrutinib group (6% vs 1%, all grades; 2% vs 0%, grade ≥3).5 With extended follow-up of 21 months, 10% and 4% of ibrutinib-treated patients had developed any grade or grade ≥3 atrial fibrillation, respectively.18 A pooled analysis of 4 randomized controlled studies of ibrutinib vs comparator in patients with CLL or mantle cell lymphoma (MCL) found that atrial fibrillation was more common in ibrutinib-treated patients than control patients (6% vs 2%, all grade; 3% vs 1%, grade ≥3).11 The prevalence of atrial fibrillation was greatest during the first 3 months on therapy, although late events did occur. The median time to onset of atrial fibrillation was 2.8 months from the start of ibrutinib therapy. Sixty-nine percent had complete resolution of atrial fibrillation, and atrial fibrillation led to discontinuation in only 1% of patients treated with ibrutinib.11 In relapsed and refractory CLL patients treated with ibrutinib outside of clinical trials, the reported rate of atrial fibrillation is up to 8%.12,13 Atrial fibrillation led to treatment discontinuation in 12% of the previously treated and 25% of the previously untreated patients who required discontinuation of ibrutinib. The median time to ibrutinib discontinuation for atrial fibrillation was 7 months.10 A small study prospectively evaluated patients treated with ibrutinib and found several risk factors that may predispose patients to developing atrial fibrillation, including preexisting cardiac comorbidities and higher left atrial diameter and area as detected by echocardiography.20 In summary, ibrutinib-related atrial fibrillation is seen in up to 10% of patients treated with the drug, and this risk should be discussed with patients before initiation of therapy.
Frequency of highlighted adverse events on selected landmark ibrutinib studies
| Adverse event | Phase 2, follow-up 21 mo6 (n = 85) | Phase 3 RESONATE | Phase 3 RESONATE2 | ||
|---|---|---|---|---|---|
| Follow-up 9 mo4 (n = 195) | Follow-up 19 mo16,17 (n = 195) | Follow-up 18 mo5 (n = 135) | Follow-up 21 mo18 (n = 135) | ||
| Atrial fibrillation | |||||
| All grades | 3 (4) | 10 (5) | 13 (7) | 8 (6) | 14 (10) |
| Grade ≥3 | 0 | 6 (3) | 7 (4) | 2 (1) | 6 (4) |
| Bleeding | |||||
| All grades | 14 (16) | 86 (44) | NR | NR | 9 (7) |
| Grade ≥3 | 4 (5) | 2 (1) | 4 (2) | 6 (4) | 8 (6) |
| Infection | |||||
| All grades | NR | 137 (70) | NR | NR | NR |
| Grade ≥3 | NR | 47 (24) | 59 (30) | NR | 31 (23) |
| Arthralgia | |||||
| All grades | 23 (27) | 34 (17) | 44 (23) | 22(16) | 27 (20) |
| Grade ≥3 | 0 | 2 (1) | NR | 2 (1) | 3 (2) |
| Myalgia | |||||
| All grades | 16 (19) | 19 (10) | NR | NR | NR |
| Grade ≥3 | 1 (1) | 1 (1) | NR | NR | NR |
| Adverse event | Phase 2, follow-up 21 mo6 (n = 85) | Phase 3 RESONATE | Phase 3 RESONATE2 | ||
|---|---|---|---|---|---|
| Follow-up 9 mo4 (n = 195) | Follow-up 19 mo16,17 (n = 195) | Follow-up 18 mo5 (n = 135) | Follow-up 21 mo18 (n = 135) | ||
| Atrial fibrillation | |||||
| All grades | 3 (4) | 10 (5) | 13 (7) | 8 (6) | 14 (10) |
| Grade ≥3 | 0 | 6 (3) | 7 (4) | 2 (1) | 6 (4) |
| Bleeding | |||||
| All grades | 14 (16) | 86 (44) | NR | NR | 9 (7) |
| Grade ≥3 | 4 (5) | 2 (1) | 4 (2) | 6 (4) | 8 (6) |
| Infection | |||||
| All grades | NR | 137 (70) | NR | NR | NR |
| Grade ≥3 | NR | 47 (24) | 59 (30) | NR | 31 (23) |
| Arthralgia | |||||
| All grades | 23 (27) | 34 (17) | 44 (23) | 22(16) | 27 (20) |
| Grade ≥3 | 0 | 2 (1) | NR | 2 (1) | 3 (2) |
| Myalgia | |||||
| All grades | 16 (19) | 19 (10) | NR | NR | NR |
| Grade ≥3 | 1 (1) | 1 (1) | NR | NR | NR |
Values represent number (percentage) of patients.
NR, not reported.
Mechanism of atrial fibrillation
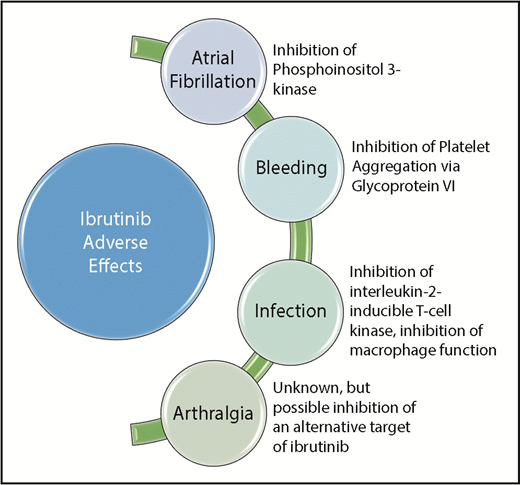
The mechanism of ibrutinib-induced atrial fibrillation remains unknown. One group showed that in mice treated with ibrutinib, the generation of arrhythmias was dose dependent, suggesting an alternative target of the drug as the cause for arrhythmogenesis.21 A proposed mechanism is the off-target inhibition of cardiac phosphoinositide 3-kinase (PI3K; Figure 1). One group found that mice with decreased cardiac PI3K activity were very susceptible to atrial fibrillation.22,23 This group also studied human cardiac samples and found that patients with atrial fibrillation had reduced cardiac PI3K activity when compared with patients without atrial fibrillation.22,23 Another group found that chronic ibrutinib exposure in mice and rabbits led to prolonged cardiac action potentials and markedly increased cardiac late sodium current. These effects were reversible with infusion of phosphatidylinositol (3,4,5)-triphosphate, an effector of PI3K, which further supports the role of PI3K inhibition in cardiac arrhythmogenesis.24 Further investigation is needed in this area, as life-threatening ventricular arrhythmias have also been reported with ibrutinib use.25
Frequency of bleeding events
A review of patients treated with ibrutinib in clinical trials and clinical practice reveals a risk of minor bleeding in up to 66% of patients and a risk of major bleeding in up to 6% of patients (Table 1).4,6,17,18 In the landmark phase 2 study where 85 patients with relapsed or refractory CLL were treated with ibrutinib, 16% of patients experienced bleeding of any grade, and 5% experienced bleeding grade ≥3.6 During the same time period, in a study of ibrutinib in 111 patients with relapsed and refractory mantle cell lymphoma, grade ≥3 bleeding was seen in 5% of patients.26 Of 4 patients with subdural hematomas, all were receiving either warfarin or aspirin.26 As such, subsequent ibrutinib studies excluded patients receiving warfarin. In the phase 3 RESONATE study for patients with relapsed CLL, bleeding of any grade, including petechiae and ecchymoses, was more common in patients receiving ibrutinib vs ofatumumab (44% vs 12%, respectively).4 Major hemorrhage (requiring hospitalization or blood transfusion) occurred in 1% of patients (n = 2) treated with ibrutinib vs 2% of patients treated with ofatumumab.4 With extended follow-up of 19 months, only 2 additional cases (4%) of major hemorrhage were reported in ibrutinib-treated patients.16 In the phase 3 RESONATE2 study for patients with previously untreated CLL, major hemorrhage (grade ≥3 or involving the central nervous system) occurred in 4% of patients (n = 6) receiving ibrutinib compared with 2% of patients (n = 3) receiving chlorambucil.5 With extended follow-up of 21 months, only 2 additional cases (6%) of major hemorrhage were reported in ibrutinib-treated patients.18 In 2 large pooled analyses of clinical trials where patients received ibrutinib vs a competitor, low-grade bleeding was reported in 35% of the ibrutinib-treated vs 12% to 15% in the competitor-treated patient groups.11,27 However, both analyses found that the risk of major hemorrhage was no different between the 2 groups.11,27 Median time to onset of major hemorrhage was 6 months.11 In a real-world analysis, 70 ibrutinib-treated patients were retrospectively analyzed. The group found that 56% of patients had grade 1 or 2 events and 19% had grade ≥3 events, which is higher than previously reported in the clinical trial setting.28 Of those patients with major bleeding, most were concurrently taking an antiplatelet agent (70%) or an anticoagulant (17%), with 13% taking both antiplatelet and anticoagulant medications. The concurrent use of ibrutinib and both antiplatelet and anticoagulant therapy significantly increased the risk of a major bleeding event (hazard ratio, 19.2; 95% confidence interval, 2.3-166.7; P < .01).28 In summary, minor bleeding events are common in ibrutinib-treated patients, and major events are less common but may be provoked by concurrent use of ibrutinib and anticoagulation or antiplatelet agents. Patients should be counseled about the risk of bleeding upon initiation of ibrutinib. This includes instructions to hold ibrutinib for 3 days before and after minor surgical procedures and 7 days before and after major surgical procedures.
Mechanism of bleeding
Bleeding seen in patients treated with ibrutinib is believed to be due to both on-target and alternative-target kinase inhibition (Figure 1). BTK, along with other members of the Tec family of kinases, has a known role in platelet aggregation via glycoprotein VI signaling.29-31 In vitro studies of BTK inhibition by ibrutinib in blood collected from CLL and MCL patients confirmed reduced platelet signaling and functions downstream of glycoprotein VI, which strongly affected firm platelet adhesion on von Willebrand factor under arterial flow.32 The same group reported that collagen-mediated platelet aggregation was reduced in blood from ibrutinib-treated patients.32,33 This effect was correlated with bleeding events and reversed with ibrutinib discontinuation.32,33 As platelets do not synthesize new BTK and ibrutinib’s half-life is short (4-6 hours), the group’s research suggests that platelet transfusion may restore normal hemostasis during bleeding events.32-34 In summary, on-target BTK and off-target Tec kinase inhibition by ibrutinib are responsible for bleeding events seen in patients, which can be reversed with cessation of ibrutinib and/or platelet transfusion.
Suggested management of atrial fibrillation and bleeding events
Atrial fibrillation
Management of atrial fibrillation of a CLL patient receiving ibrutinib therapy requires collaboration between the hematologist and cardiologist with consideration of the patient’s individual risk of stroke vs competing risk of bleeding (Figure 2). Atrial fibrillation and its associated anticoagulation present a particular challenge to the practicing clinician given the impaired hemostasis caused by ibrutinib. When a patient is diagnosed with atrial fibrillation, we suggest consultation with a cardiologist for comanagement of these complex cases. Rate and/or rhythm control should be achieved. It should be noted that diltiazem, verapamil, and amiodarone are inhibitors of CYP3A4, which is a primary site for ibrutinib metabolism, and concurrent use may increase serum ibrutinib concentration and toxicity.35 Additionally, serum amiodarone concentration may be increased secondary to ibrutinib’s inhibition of P-glycoprotein, leading to increased toxicity.35 In addition to rate and/or rhythm control, we suggest using a validated tool to estimate the patient’s risk of stroke. We use the CHA2DS2-VASc risk stratification tool, where 1 point each is assigned to patients with a history of congestive heart failure, hypertension, diabetes mellitus, vascular disease, age 65 to 74 years, or female sex and 2 points are assigned to patients age ≥75 years or with a history of stroke, for a maximum score of 9 points.36 If a patients score is 0 to 1 on this scale, then their risk of stroke is <1% per year.36 A score of ≥2 on this scale is associated with at least 2% per year risk of stroke from atrial fibrillation.36 However, it is notable that this score is merely an estimate of the patient’s risk for thromboembolic events, as it has not been validated specifically in CLL patients. While a similar risk score has reportedly underestimated the risk of thromboembolic events in cancer patients,15 a series of 76 ibrutinib-treated patients with atrial fibrillation from our institution had only 1 thromboembolic episode despite recommended anticoagulation in only 29% of these cases. In our series, bleeding was more problematic than thrombosis for this patient population.37 We consider a CHA2DS2-VASc score of ≥2 to denote a considerable risk of thromboembolic events. As such, if a patient is assigned a CHA2DS2-VASc score of ≥2, then anticoagulation is recommended. We suggest that ibrutinib should be discontinued and alternate therapy for CLL should be initiated. Similarly, if an unprovoked, initial atrial fibrillation or significant ventricular tachycardia event occurs during the first 3 months of treatment or is recurrent at any point in the treatment, then we discontinue ibrutinib. If a patient is assigned a CHA2DS2-VASc score of 0 to 1, then anticoagulation is not required, although the risk of thromboembolic events should be discussed with the patient. In this case, we suggest continuing ibrutinib. We do not consider a previous diagnosis of atrial fibrillation or other cardiac arrhythmia a contraindication to ibrutinib initiation. However, novel agents such as acalabrutinib, a more specific BTK inhibitor, may have a lower frequency of atrial fibrillation and will be one option in this setting in the United States, where it is approved for marketing in MCL and listed in the National Comprehensive Cancer Network guidelines for relapsed CLL.38
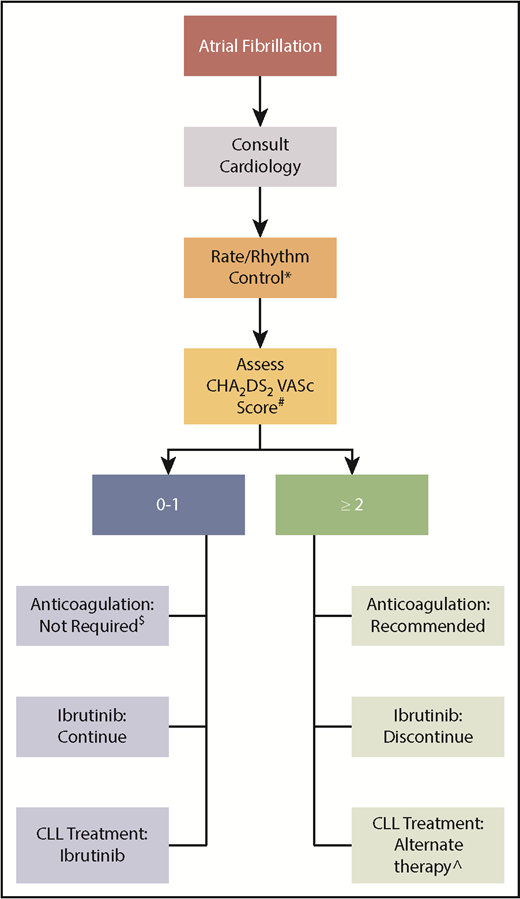
Management of atrial fibrillation in patients treated with ibrutinib. *Notable drug interactions with ibrutinib include diltiazem, verapamil, and amiodarone (CYP3A4 inhibitors) and amiodarone (P-glycoprotein). #1 point each for a history of congestive heart failure, hypertension, diabetes mellitus, or vascular disease, age 65 to 74 years, or female sex and 2 points each for age ≥75 years or a history of stroke. $Discuss risk of thromboembolic events with patient. ^Possible options include venetoclax with or without rituximab, idelalisib, and duvelisib.
Management of atrial fibrillation in patients treated with ibrutinib. *Notable drug interactions with ibrutinib include diltiazem, verapamil, and amiodarone (CYP3A4 inhibitors) and amiodarone (P-glycoprotein). #1 point each for a history of congestive heart failure, hypertension, diabetes mellitus, or vascular disease, age 65 to 74 years, or female sex and 2 points each for age ≥75 years or a history of stroke. $Discuss risk of thromboembolic events with patient. ^Possible options include venetoclax with or without rituximab, idelalisib, and duvelisib.
Anticoagulation and bleeding events
The concurrent use of ibrutinib and anticoagulants is not recommended secondary to increased risk of bleeding. Regarding warfarin, because some patients on early studies who were concurrently on ibrutinib and warfarin experienced major bleeding events, and because subsequent ibrutinib studies excluded patients taking warfarin, we do not recommend the concurrent use of warfarin and ibrutinib.26 Regarding direct thrombin inhibitors, there are interactions between ibrutinib and apixaban and rivaroxaban via CYP3A interaction and between ibrutinib and dabigatran through P-glycoprotein interaction.39 These interactions can lead to increased bleeding risk, and we do not recommend concurrent use of these agents. If immediate anticoagulation is required and no alternate therapies for CLL are available, then we recommend anticoagulation with enoxaparin (off-label indication) and careful maintenance of platelets over 50 × 109/L. Patients should be educated about their bleeding risk. In the event that a major bleeding event occurs in a patient receiving ibrutinib therapy, we recommend discontinuing ibrutinib and transfusing the patients with platelets until clinical evidence of bleeding resolves.
Summary of case 1
After diagnosis of atrial fibrillation, the patient was started on metoprolol, which is an appropriate choice without interactions with ibrutinib. The patient’s CHA2DS2-VASc score was 3 for advanced age and history of vascular disease, and we agree that anticoagulation should be initiated to prevent the risk of stroke. However, we strongly disagree with placing the patient on concurrent warfarin and ibrutinib. In this case, we would have recommended discontinuation of ibrutinib and a switch to an alternative therapy, such as venetoclax with or without rituximab, idelalisib, or duvelisib, which have a lower reported incidence of atrial fibrillation and bleeding risk.40-42 For treatment of this patient’s large retroperitoneal bleed, we recommend discontinuation of ibrutinib, transfusion of platelets to counteract the effects of ibrutinib on the platelets, and transfusion of fresh frozen plasma and administration of vitamin K to reverse the effects of warfarin. After stabilization of the retroperitoneal bleed, anticoagulation may be considered at a later date for the underlying risk of significant thromboembolic disease.
Case 2: infection
The patient is a 66-year-old female with CLL who was treated with fludarabine, cyclophosphamide, and rituximab therapy 3 years ago. She achieved complete remission to therapy, but since that time, she has had 5 episodes of autoimmune hemolytic anemia, which resolved after treatment with prolonged prednisone tapers. Four months ago, she began treatment with ibrutinib 420 mg daily secondary to progressive B-symptoms and bulky lymphadenopathy. She presented with a 1-month history of nonproductive cough, fatigue, low-grade fevers, and dyspnea. She saw her primary care physician 3 weeks ago and completed a course of antibiotics, with no improvement in her symptoms. Chest radiograph showed bilateral patchy infiltrates. Computed tomography showed bilateral patchy consolidations with air bronchograms and multiple small cavitary lesions. Bronchoscopy revealed Aspergillus fumigatus.
Frequency of infections
A review of clinical trials of CLL patients treated with ibrutinib reveals an increased rate of infections, most notably pneumonia. In the phase 2 study of 85 relapsed CLL patients treated with single-agent ibrutinib, upper respiratory tract infections of any grade were reported in 33% of patients. Grade ≥3 pneumonia was reported in 12%. Serious infections were more commonly reported early in the ibrutinib treatment course. The average infection rate of infection was 7.1 per 100 patient-months during the first 6 months of ibrutinib treatment and 2.6 per 100 patient-months thereafter.6 In the phase 3 RESONATE study, 70% of the 195 relapsed CLL patients who received ibrutinib reported any grade of infection with 24% reporting infections grade ≥3.4 With extended follow-up of 19 months, 30% of ibrutinib-treated patients developed infections grade ≥3.17 It is notable that the incidence of infection decreased over time during ibrutinib therapy.16 In the phase 3 RESONATE2 study, 23% of previously untreated CLL patients who received ibrutinib reported infections grade ≥3, with the incidence of these infections decreasing over time.18 A pooled analysis of 4 randomized controlled studies of ibrutinib vs comparator in patients with CLL or MCL found that grade ≥3 pneumonia was more common in ibrutinib-treated patients than in those treated with the comparator (8% vs 6%).11 In patients receiving ibrutinib, the risk of infections was greatest during the first 3 months of therapy (41%, all grade; 11%, grade 3/4) and decreased over time.11,43 A large meta-analysis of ibrutinib-treated patients who participated in published clinical trials found that 56% of patients had an infectious complication and that 1 of every 5 patients developed pneumonia.44 In a real-world retrospective analysis of ibrutinib-treated patients, infection led to treatment discontinuation in 11% of the previously patients who required discontinuation of ibrutinib. The median time to ibrutinib discontinuation for infection was 6 months.10 In summary, infection is common and notably more frequent early in the course of ibrutinib therapy.
A specific infection of particular concern in ibrutinib-treated patients is Aspergillus fumigatus. A clear risk of A fumigatus infection was identified in a clinical trial for patients with primary central nervous system lymphoma who received ibrutinib in combination with chemoimmunotherapy and steroids. In this study, 7 of the 18 treated patients (39%) developed infections with A fumigatus, including 2 patient deaths related to the infection.45 The incidence of A fumigatus infection in other lymphoid malignancies is likely lower than seen and has been reported as 2.5% in a large retrospective study of 566 patients treated at a single institution.46 However, if an invasive fungal infection develops in an ibrutinib-treated patient, then A fumigatus may be the most likely causative agent. A retrospective study of 33 ibrutinib-treated patients at a single center who developed invasive fungal infections found Aspergillus to be the causative agent in 27 (81%).47 Particular risk factors for this infection have been identified, including concurrent corticosteroids, many prior cancer treatments, diabetes, and liver disease.45,46,48 As such, physicians should have a high index of suspicion for aspergillosis if a fungal infection is detected in an ibrutinib-treated patient.
Another specific infection of potential concern is Pneumocystis jirovecii. One center reported 5 cases of P jirovecii pneumonia (PCP) in 96 CLL patients receiving ibrutinib on clinical trials at their institution. The median time from initiation of ibrutinib to PCP was 6 months (range, 2-24 months). The estimated incidence of PCP in this series was 2 cases per 100 patient-years.49 Four of the 5 cases had previously untreated CLL, indicating that infectious risk was not related to immunosuppression from prior therapies. Interestingly, the reported rate of PCP is much lower in patients receiving ibrutinib to treat other hematologic malignancies, which may indicate that the risk of infection is related to immunosuppression from the underlying disease as opposed to the drug itself.50 However, a thorough evaluation of all suspected fungal infections is necessary to determine etiology and optimal treatment.
Mechanism of infections
There are several postulated mechanisms explaining the increased risk of infection in patients treated with ibrutinib (Figure 1). One theory identified ibrutinib’s off-target inhibition of interleukin-2–inducible T-cell kinase with impairment of immune function.51 Another group cited inhibition of natural killer cell antibody-dependent cellular cytotoxicity as a potential mechanism of immune impairment.52 Data from another group implicated reduced macrophage phagocytosis in ibrutinib-treated human cells.53 It is likely that there is an interplay of multiple effects of ibrutinib that lead to increased infections in patients treated with the agent. It is also notable that infections were more frequent during the first few months on ibrutinib therapy as described above. Based on this fact, one hypothesis is that immune deficiencies related to the CLL, such as hypogammaglobulinemia, may be more responsible for infectious risk than treatment with ibrutinib. After continuous ibrutinib therapy, there are data to support reconstitution of both cellular (diversification of the T-cell compartment) and humoral (sustained increase in immunoglobulin A levels) immunity, leading to decreased rate of infections over time.54,55
Specifically regarding the increased risk of A fumigatus infections in patients treated with ibrutinib, several studies in animal models have pointed to potential mechanisms for these infections. One group found that BTK is necessary for the activation of macrophages, which clear the airways of the pathogen.56 Another group showed that BTK knockout mice infected with A fumigatus exhibited greater mortality, greater weight loss, more severe lung tissue damage, and a higher fungal burden than the mice with functional BTK.45 A study in human macrophages reveals that BTK blockade with ibrutinib inhibits nuclear translocation of NFAT and NF-κB (critical to neutrophil recruitment), prevents production of tumor necrosis factor-α and inhibits galactomannan production.48,57 The sum of these findings indicates that patients receiving ibrutinib may be more susceptible to infections with A fumigatus secondary to inhibition of macrophage responses.
Suggested management of infections
For infections of grade 4, ibrutinib should be held until infection is appropriately treated and has resolved to at least grade 3. For infections of grade 1 to 3, we recommend continuing ibrutinib therapy and treating the infection with appropriate anti-infective agents with careful attention to drug interactions with ibrutinib. The management of fungal infections while the patient receives ibrutinib therapy is particularly challenging secondary to drug interactions. For example, the optimal management of aspergillosis includes the use of -azole therapies such as voriconazole, posaconazole, or iatraconazole. Unfortunately, these are all strong inhibitors of CYP3A4, which are not recommended in combination with ibrutinib, as it could significantly increase the serum concentrations of ibrutinib and risk for toxicity. These drug interactions are of particular concern as the recommended course of therapy for fungal infections such as aspergillosis is prolonged. Amphotericin B and echinocandins, such as caspofungin, can be used safely with ibrutinib but are only available in intravenous formulation and have their own associated toxicities. In scenarios where strong inhibitors of CYP3A4 need to be used in combination with ibrutinib, a reduced dose of ibrutinib is indicated along with careful clinical monitoring for toxicity. In regards to prophylaxis for infection, no antifungal or antibacterial agents are currently recommended while a patient is treated with ibrutinib. Due to the higher risk of Varicella zoster in CLL in general, we often administer prophylactic acyclovir or valacyclovir in ibrutinib-treated patients.
Summary of case 2
Our patient had several risk factors for A fumigatus infection, including prolonged corticosteroid therapy for autoimmune hemolytic anemia, prior immunosuppressive therapy for CLL, and ibrutinib therapy. Ibrutinib treatment may have inhibited her intrinsic macrophage function, making her airways particularly susceptible to A fumigatus infection. After consultation with an infectious disease specialist, our patient was treated with a voriconazole load IV for 7 days and then transitioned to voriconazole orally at a dose of 200 mg twice daily. Ibrutinib therapy was held during the 7 days of IV voriconazole and then resumed at a dose of 140 mg daily on day 8 of aspergillosis therapy. Careful clinical monitoring for ibrutinib toxicity was performed.
Case 3: arthralgia
The patient is a 60-year-old male carpenter with recently diagnosed high-molecular-risk CLL (unmutated immunoglobulin heavy-chain gene and del(17)(p13.1) by karyotype) who presented with severe fatigue, anemia, and thrombocytopenia. There was no evidence of hemolysis, and bone marrow was consistent with 90% involvement of CLL. Secondary to a high molecular risk, he was started on ibrutinib 420 mg daily 3 months ago. He presents with diffuse joint pain that is preventing him from functioning at his job.
Frequency of arthralgia
Review of clinical trials on which CLL patients were treated with ibrutinib reveals an increased rate of arthralgia and myalgia (Table 1). The early phase 2 study in which 85 patients with relapsed CLL were treated with single-agent ibrutinib demonstrated that 27% and 19% experienced any grade of arthralgia or myalgia, respectively, while 1% experienced grade ≥3 arthralgia and myalgia.6 In the phase 3 RESONATE study, relapsed CLL patients receiving ibrutinib had an increased rate of any grade of arthralgia compared with patients receiving ofatumumab (17% vs 7%).4 With extended follow-up of 19 months, 23% of ibrutinib-treated patients developed arthralgias, indicating a decreased incidence over time.16 Similarly, in the phase 3 RESONATE2 study, previously untreated CLL patients receiving ibrutinib had an increased rate of any grade of arthralgia compared with patients receiving chlorambucil (16% vs 7%).5 With extended follow-up of 21 months, 20% of ibrutinib-treated patients developed arthralgias, indicating a decreased incidence over time.18 A pooled analysis of 4 randomized controlled studies of ibrutinib vs comparator in patients with CLL or MCL found that any-grade arthralgia was more common in ibrutinib-treated patients than those treated with the comparator (13% vs 8%).11 In a real-world retrospective analysis of ibrutinib-treated patients who required treatment discontinuation, arthralgia was the most common toxicity leading to treatment discontinuation in 42% of the previously untreated patients. The median time to ibrutinib discontinuation for arthralgia was 5 months.10 Although the majority of arthralgias appear to be low grade, severe cases have been reported.58 Therefore, clinicians should be aware of this frequent adverse event and its management.
Mechanism of arthralgia
There are no published data to confirm the etiology of arthralgia in ibrutinib-treated patients. Another puzzling piece is that ibrutinib was initially developed as a treatment of rheumatoid arthritis and has demonstrated significant efficacy in murine models of rheumatoid arthritis.59 The causative mechanism for this arthralgia is also unknown but may be due to an alternative kinase target of ibrutinib, as this complication is often less frequent with more specific, irreversible inhibitors such as acalabrutinib38 (Figure 1).
Suggested management of arthralgia
In our clinical experience, the arthralgia experienced in ibrutinib-treated patients is more pronounced early in the treatment course and can resolve on its own over months even without discontinuing ibrutinib therapy. In some cases, it can also come on late and be very disruptive to patient quality of life. When managing ibrutinib-associated arthralgia, the use of anti-inflammatory agents with antiplatelet adverse events, such as ibuprofen, should be avoided if possible secondary to bleeding risk when used concurrently with ibrutinib. We suggest the use of acetaminophen or short pulses of prednisone therapy and continuing ibrutinib at full dose and have found that once the patient has been on ibrutinib therapy for ≥6 months, the arthralgias abate on their own. After this, an anti-inflammatory agent such as ibuprofen can be initiated. If the patient cannot tolerate the arthralgia, then we suggest holding the dose of ibrutinib for up to a week to allow symptoms to resolve and reduction of the dose by 1 dose level (for example, 420 mg to 280 mg). In some cases, transition to an alternative BTK inhibitor such as acalabrutinib can result in diminishment or resolution of this adverse effect.60
Summary of case 3
Our patient experienced severe arthralgia early in the course of ibrutinib therapy. As his symptoms were interfering with his day-to-day life, we recommended a 5-day course of tapered corticosteroids (Medrol pack), which led to significant improvement of his symptoms that lasted 2 to 3 weeks before recurrence of severe symptoms. At that time, we held the ibrutinib for 7 days, which allowed for resolution of his arthralgia, and restarted him at a reduced dose of 280 mg. He has tolerated this dose of ibrutinib and has experience a significant improvement in CLL-related symptoms and cytopenias. Had this persisted, we would have considered changing his treatment to acalabrutinib or venetoclax with or without rituximab.
Additional adverse events of interest
In this article, we have thoroughly reviewed select adverse effects that require specific and specialized management. In this section, we will briefly review additional ibrutinib-related adverse events of interest, including diarrhea, dermatologic events, hypertension, and pneumonitis.
Diarrhea
Diarrhea is the most common ibrutinib-related adverse effect and is seen in ∼50% of patients.16-18,61 However, the diarrhea is rarely severe, with <5% reporting grade ≥3 diarrhea.16,18 The incidence of diarrhea is highest during the first 6 months of therapy (∼50%) and drops rapidly after this time point (∼5% by 18 months).16,17 The diarrhea is typically short-lived, with a reported median duration of 6 to 20 days.18,61 The proposed mechanism of action for ibrutinib-related diarrhea is off-target inhibition of epidermal growth factor receptor (EGFR), as diarrhea is a known adverse effect seen with EGFR inhibitors.62 In our experience, ibrutinib-related diarrhea is usually self-limited and resolves with no intervention or minimal dietary modifications. As infections are also common in this population, stool samples should be sent for common pathogens to rule out infection. Otherwise, patients should be counseled to stay on the medication with treatment such as loperamide, as this side effect diminishes with time. In rare cases of grade ≥3 diarrhea (≥7 stools per day over baseline or need for hospitalization), ibrutinib should be held until diarrhea resolves to at least grade 2. We would recommend resuming ibrutinib at the same dose, with the option to reduce the dose if grade ≥3 diarrhea occurs a second time.
Dermatologic events
Dermatologic events, such as skin rash, are less common but often bothersome ibrutinib-related side effects. Rash has been reported in up to 27% of CLL patients receiving ibrutinib, with the vast majority classified as low grade.6 Two common variants of the rash have been described.63 The first is a nonpalpable, nonpruritic petechial rash likely related to ibrutinib-induced platelet dysfunction as already described in this article. The second variant is a palpable, sometimes pruritic rash, which may be related to ibrutinib’s off-target inhibition of EGFR.62 In our experience, these rashes are typically self-limited and do not require ibrutinib dose holds or reductions; however, they will quickly resolve with dose holds. Patients should be counseled to stay on the medication, and topical steroids or oral antihistamines can be used in patients with pruritic symptoms. Other common concerns of patients receiving ibrutinib therapy are brittle nails and textural hair changes (softening and straightening), reported in 67% and 26% of patients treated on one study.64 These adverse events do not require holding or reducing the dose of ibrutinib. Application of oil to the cuticle bed or supplementation of biotin may aid brittle nails.64,65 We have noted many cases of thickening and tightening of skin in the lower extremities, which we refer to as “tree trunk legs.” Cessation of ibrutinib generally results in resolution of this side effect. Other rare dermatologic toxicities have been reported, and management should be tailored to the patients symptom severity and tolerance of the toxicity.66,67
Hypertension
Hypertension is another notable adverse event associated with ibrutinib treatment and has been reported in up to 20% of patients, with ∼5% noted to be grade ≥3 (≥160/110 mm Hg).6,16-18 Unlike most toxicities, the incidence of hypertension remains stable over time.17,18 The underlying mechanism for hypertension is unclear at this time. We recommend monitoring blood pressure in patients on ibrutinib. If hypertension is diagnosed, then we do not hold ibrutinib but medically manage the hypertension along with the patient’s primary care physician.
Pneumonitis
A very rare but life-threatening adverse effect associated with ibrutinib is pneumonitis.68 The mechanism for ibrutinib-associated pneumonitis is unknown. If a patient receiving ibrutinib develops progressive respiratory symptoms, then we recommend evaluation with imaging of the lungs. If imaging is abnormal, then we recommend evaluation for infection via bronchoscopic culture. If pneumonitis is suspected, then the patient should receive systemic corticosteroids until clinical and radiological resolution of the symptoms. For ibrutinib-induced pneumonitis, we recommend permanent discontinuation of ibrutinib and selection of alternative CLL therapy for the patient.
General recommendations
For the adverse events not specifically mentioned here, clinicians can follow the general recommendations for dose holds or reductions described in the package insert. The insert recommends holding ibrutinib for any grade ≥3 nonhematologic toxicities, grade ≥3 neutropenia with infection or fever, or grade 4 hematologic toxicities. The drug should be held until the toxicity recovers to grade 1 or baseline. After the first hold, the drug can be resumed at the same dose. After the second or third holds, ibrutinib can be reduced by 1 dose level. If a fourth hold is required, then ibrutinib should be discontinued and alternate therapy for CLL started. When managing ibrutinib-related toxicities, a dedicated clinical pharmacist can be helpful to review any new medications for interactions with ibrutinib, with careful attention to CYP3A4 metabolism. It should be noted that prolonged ibrutinib interruption is typically associated with a flare of CLL-related symptoms and has been associated with a shorter median progression-free survival in CLL patients.69 Although not extensively studied, there are some data to support similar clinical efficacy with reduced ibrutinib doses.70,71 There are some theoretical concerns that holding or reducing ibrutinib could promote resistance to therapy. As such, a patient who develops ibrutinib-related adverse effects should be evaluated by their treating physician and have a thorough discussion about the risks and benefits of holding or reducing ibrutinib vs switching to an alternative CLL therapy.
Conclusions
Ibrutinib is highly efficacious for the treatment of CLL; however, ibrutinib-related adverse events are common and have resulted in discontinuation of therapy in >20% of patients taking the drug in a real-world setting.10 In this article, we have reviewed adverse effects that require specific and specialized management but do not have the ability to address every adverse effect reported with ibrutinib. There are some adverse effects in which the management does not always require dose holds or reductions, such as arthralgia or hypertension. In contrast, there are some adverse events that nearly always require discontinuation of ibrutinib, such as the need for anticoagulation with warfarin or drug-induced pneumonitis. The incidence of the majority of adverse events decreases over time, and many patients are able to remain on ibrutinib therapy with management by the treating physician. In summary, the prescribing hematologist should be aware of common ibrutinib-related adverse events and educate their patients before starting therapy. These adverse events should be managed with careful consideration of drug interactions and with the assistance of a clinical pharmacist and consulting subspecialists as needed. The risks and benefits of continuing ibrutinib vs changing to an alternate CLL therapy should be reviewed with the patient, and an educated decision should be made for each individual patient.
Acknowledgments
The authors thank the many patients who have received ibrutinib and informed their strategy for managing adverse events arising from this highly impactful therapy.
J.C.B. is supported by the Four Winds Foundation, D. Warren Brown Foundation, Mr. and Mrs. Michael Thomas, the Sullivan CLL Research Foundation, and the National Institutes of Health, National Cancer Institute (R35 CA197734). D.M.S. is supported by the National Institutes of Health, National Cancer Institute (K23 CA212271‐01).
Authorship
Contribution: D.M.S. and J.C.B. planned the sections of the paper through several detailed discussions; D.M.S. drafted the initial version of this paper, followed by detailed editing and discussion between both authors; and D.M.S. and J.C.B. approved the final manuscript.
Conflict-of-interest disclosure: J.C.B. has received research funding from Acerta Pharma, Genentech, Janssen, Verestem, and Pharmacyclics and is or has been a consultant (<$5000) for Acerta Pharma, Pharmacyclics, Jazz Pharmaceuticals, Gilead Pharmaceuticals, and Verastem Pharmaceutics for advice on drug development. D.M.S. has received research funding from the Lymphoma Research Foundation, Acerta Pharma, and Gilead and honoraria from Genentech.
Correspondence: John C. Byrd, 455B OSUCCC, 410 West 12th Ave, The Ohio State University, Columbus, OH 43210; e-mail: john.byrd@osumc.edu; and Deborah M. Stephens, D.O. 2000 Circle of Hope, Research South 5509, University of Utah, Huntsman Cancer Institute, Salt Lake City, UT 84112; e-mail: deborah.stephens@hci.utah.edu.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal