

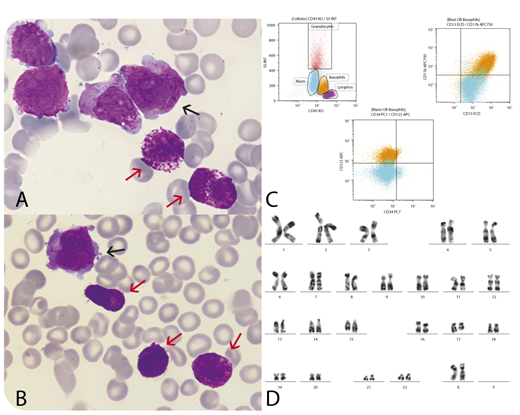
A 59-year-old woman was hospitalized for investigation of spontaneous bruises on arms and legs and asthenia. Complete blood count and blood smear review showed pancytopenia (platelets 78 × 109/L, hemoglobin concentration 10.6 g/dL, leukocytes 1.8 × 109/L) with 10% blast cells and 13% basophils (0.2 × 109/L). Coagulation tests, including fibrinogen and D-dimers, were normal. Bone marrow examination showed 64% hypergranular blasts with Auer rods (panels A and B, black arrows; original magnification ×100, May-Grünwald Giemsa stain), typical of acute promyelocytic leukemia (APL) and 13% basophils with abnormal features: hypergranularity and abnormal granular repartition (red arrows). Flow cytometry (panel C) confirmed a typical profile of promyelocytic cells (cMPO+, CD34−, HLA DR−, CD117+, CD33+, CD13+, CD123−) and basophils (CD11b+, CD25+, CD123+, CD13+, CD33+, CD44+) with an abnormal immunophenotypic profile (CD38−, CD117low). Cytogenetic analysis (panel D) revealed t(15;17)(q24;q21), and molecular analysis showed classical PML-RARA transcript. Classical APL treatment was given. Basophilia increased to 0.39 ×109/L at day 19 and normalized by day 24. The patient has started her first consolidation without problems.
Basophilia at diagnosis of APL is very uncommon. This case highlights that basophilia can be associated with an APL clone. Basophilia at presentation of APL has been reported and said to have an increased risk of bleeding, not seen in this patient.
A 59-year-old woman was hospitalized for investigation of spontaneous bruises on arms and legs and asthenia. Complete blood count and blood smear review showed pancytopenia (platelets 78 × 109/L, hemoglobin concentration 10.6 g/dL, leukocytes 1.8 × 109/L) with 10% blast cells and 13% basophils (0.2 × 109/L). Coagulation tests, including fibrinogen and D-dimers, were normal. Bone marrow examination showed 64% hypergranular blasts with Auer rods (panels A and B, black arrows; original magnification ×100, May-Grünwald Giemsa stain), typical of acute promyelocytic leukemia (APL) and 13% basophils with abnormal features: hypergranularity and abnormal granular repartition (red arrows). Flow cytometry (panel C) confirmed a typical profile of promyelocytic cells (cMPO+, CD34−, HLA DR−, CD117+, CD33+, CD13+, CD123−) and basophils (CD11b+, CD25+, CD123+, CD13+, CD33+, CD44+) with an abnormal immunophenotypic profile (CD38−, CD117low). Cytogenetic analysis (panel D) revealed t(15;17)(q24;q21), and molecular analysis showed classical PML-RARA transcript. Classical APL treatment was given. Basophilia increased to 0.39 ×109/L at day 19 and normalized by day 24. The patient has started her first consolidation without problems.
Basophilia at diagnosis of APL is very uncommon. This case highlights that basophilia can be associated with an APL clone. Basophilia at presentation of APL has been reported and said to have an increased risk of bleeding, not seen in this patient.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal