

Abstract
Lenalidomide and azacitidine each have activity in myelodysplastic syndromes (MDS) patients, where both microenvironment and cell-regulatory mechanisms contribute to disease pathogenesis. The objective of this multicenter, phase 2 expansion trial was to determine the efficacy and safety of combination therapy with azacitidine (75 mg/m2/d for 5 days) and lenalidomide (10 mg/d for 21 days; 28-day cycle) in patients with higher-risk MDS. Among 36 patients enrolled (18 phase 1, 18 phase 2), median age was 68 years (range, 47-78 years) and follow-up was 12 months (range, 3-55 years). IPSS categories included intermediate-1 (n = 5 patients with excess blasts), intermediate-2 (20), and high (11). Common grade 3/4 nonhematologic adverse events included febrile neutropenia (22% of patients), other infection (11%), pulmonary (11%), cardiac (11%), constitutional (11%), and dermatologic (11%). The overall response rate (per modified MDS International Working Group criteria) was 72%: 16 patients (44%) achieved a complete response (CR), and 10 (28%) had hematologic improvement. Median CR duration was 17+ months (range, 3-39+); median overall survival was 37+ months (range, 7-55+) for CR patients, and 13.6 months for the entire cohort (range, 3-55). TET2/DNMT3A/IDH1/2 mutational status was associated with response in a limited number of patients. The lenalidomide/azacitidine combination is well-tolerated and highly active in treating greater-risk MDS. This study is registered at http://www.clinicaltrials.gov as NCT00352001.
Introduction
The myelodysplastic syndromes (MDS) are a heterogeneous collection of bone marrow failure disorders associated with truncated survival because of disease-associated cytopenias, consequent bleeding and infections, and leukemic transformation, particularly in higher-risk subtypes (commonly defined as patients with excess myeloblasts or an International Prognostic Scoring System [IPSS] risk score > 1.0).1,2 Approximately 25%-30% of recently diagnosed and 15%-20% of established patients have higher-risk MDS.3
Three drugs have been approved by the US Food and Drug Administration for the treatment of MDS.4-6 Lenalidomide is used primarily in lower-risk patients with the del(5q) cytogenetic abnormality and purportedly works by selectively suppressing del(5q) clones by inhibiting haplodeficient phosphatases encoded within or near the proximal common deleted region that serves to release progenitors from p53 arrest followed by terminal arrest and apoptosis at G2/M, in association with a defect in ribosomal protein function.7-9 In patients without this lesion, lenalidomide has multiple effects that range from modulation of the bone marrow microenvironment, inhibition of lysine demethylase, and potentiation of erythropoietin signaling.10-12 Lenalidomide has demonstrated transfusion-independence response rates of 67% in lower-risk, transfusion-dependent del(5q) patients with MDS; 26% in lower-risk patients without del(5q); and 14% and 30% in older patients with acute myeloid leukemia (AML) with or without the del(5q) abnormality, respectively.5,13-16 Another drug, azacitidine, is used primarily in patients with higher-risk MDS and works through the proteosomic destruction of DNA methyltransferase and resultant chromatin decondensation.17,18 Each drug can improve peripheral cytopenias and transfusion needs in responding patients,4,6 and azacitidine improves overall survival (OS) in patients with higher-risk MDS compared with those treated with conventional care regimens.19
A phase 1 study of azacitidine in combination with lenalidomide in patients with higher-risk MDS was conducted to evaluate the possible in vivo synergism that could be achieved by targeting both the microenvironment and cell-regulatory mechanisms that likely play a role in evolution of the disease.20 Phase 2 dosing was established as azacitidine 75 mg/m2 daily for 5 days and lenalidomide 10 mg daily for 21 days of a 28-day cycle. In this phase 2 continuation study, we explored the efficacy and safety of combination therapy with azacitidine and lenalidomide in patients with higher-risk MDS and identified molecular predictors of response.
Methods
Study design
This was a multicenter, single-arm, open-label phase 2 continuation study of combination therapy with lenalidomide and azacitidine. The study received local institutional review board approval from all participating sites and from the Data Safety and Monitoring Board of the Rare Diseases Branch of the National Institutes of Health, and was registered with ClinicalTrials.gov (NCT00352001). In addition, the study was conducted in accordance with the Declaration of Helsinki. The phase 1 study was open from May 2005 through May 2008, with results already published, and the phase 2 study from March 2009 through April 2011, with results reported through February 2012. The present study includes patients from both the phase 1 and phase 2 studies.
The primary objective was to determine the safety and efficacy of combination therapy in patients with higher-risk MDS with efficacy as defined by 2006 International Working Group (IWG) criteria.21 The combination of azacitidine and lenalidomide was determined on the basis of presumed nonoverlapping mechanisms of action. Patients received up to 7 cycles of combination therapy, with patients in the phase 1 study treated with either 5- or 10-day azacitidine schedules (75 mg/m2 daily) and lenalidomide at 5 mg or 10 mg daily for 14 days or 10 mg daily for 21 days of a 28-day cycle. In the phase 2 dosing, patients followed a schedule of azacitidine 75 mg/m2 daily for 5 days and lenalidomide 10 mg daily for 21 days and could continue on single-agent azacitidine off-study thereafter. Each cycle lasted 28 days.
Patients
Patients were enrolled from all participating institutions. Subjects were > 18 years of age and had MDS of one of the following World Health Organization (WHO) classifications: chronic myelomonocytic leukemia-2; refractory anemia with excess blasts-1 (RAEB-1); or refractory anemia with excess blasts-2 (RAEB-2).22 Patients with RAEB in transformation were excluded because the WHO now defines these patients as having AML and by design the study was limited to patients with MDS because results from the azacitidine survival study were not yet available.23 Alternatively, subjects could have an IPSS score1 of intermediate-2 (1.5-2.0 points) or high (> 2.5 points) regardless of their percentage of myeloblasts. Subjects had to have an Eastern Clinical Oncology Group status < 2 and not be candidates for hematopoietic stem cell transplantation for first-line therapy, to the extent that adverse events and efficacy of the drug combination could be assessed, as indicated by patients declining this treatment option, which implied that a conversation about transplantation occurred. Initially, patients had to have a minimal platelet count of 50 000/μL, although this was amended to 20 000/μL in the fall of 2006. Patients could not use erythropoiesis-stimulating agents while on-study.
Assessment of adverse events
Adverse events were identified by use of the Common Toxicity Criteria Version 3.0. Hematologic toxicities were recorded throughout the study and are reported as mean or median percentage decreases from baseline occurring during the first 8 weeks of therapy. All subjects who received any study drug were included in analyses for safety and efficacy.
Efficacy assessment
Response was assessed using 2006 IWG MDS Response criteria after 4 cycles of therapy.21 Participants continued to receive therapy for an additional 3 cycles with stable disease; hematologic improvement (HI); complete response (CR), which included both < 5% bone marrow myeloblasts and meeting HI criteria in all 3 cell lines; or partial response.6 Response was again assessed after 7 cycles of therapy, consistent with previous publications.6 Patients were discontinued from therapy in case of relapse after CR or partial response, unacceptable toxicity, or progression of disease. Responding patients could continue on single-agent azacitidine therapy off-study per the investigator's discretion and were followed until nonresponse or disease progression; death; or study data lock (February 2012). Time to progression was from date of CR and OS from the date of study enrollment.
DNA extraction
Genomic DNA from bone marrow or whole blood was extracted by the use of Gentra Puregene DNA Extraction kit (Gentra Systems Inc) according to the manufacturer's instructions. T-lymphocytes (CD3+) were isolated by the use of immunomagnetic separation (Miltenyi Biotech) and served as germline control.
Single-nucleotide polymorphism array-based karyotyping
Single-nucleotide polymorphism array-based (SNP-A) analysis was performed on 50 ng of genomic DNA with the Affymetrix GeneChip Human Mapping 250K Array and Genome-Wide Human SNP Array 6.0 (Affymetrix) as previously described.24,25 Germline-encoded copy number variants and nonclonal areas of uniparental disomy were excluded from further analysis by the use of a bioanalytic algorithm that was determined on the basis of the results of SNP-A karyotyping in an internal control series (n = 1003) and reported in the Database of Genomic Variants.26
Mutational analysis
Genomic DNA from 19 patients enrolled at Cleveland Clinic was used for mutational analysis. Direct sequencing was performed on coding exons of TET2 (all exons), DNMT3A (exons 18-23), IDH1 (exon 4), IDH2 (exon 4), SF3B1 (exons 13-16), CBL (exons 8-9), NRAS (exons 1-2), KRAS (exons 1-2), EXZH2 (exons 18-19), U2AF1 (exons 2 and 6), SRSF2 (exon 1), and P53 (all exons). Primer sequences and conditions used are available on request. Bidirectional sequencing was performed by standard techniques with the use of the ABI 3730xl DNA analyzer (Applied Biosystems). Nonclonal CD3+ cells were used to confirm the somatic nature of the mutations. All mutations were scored as pathogenic on the basis of the observation that they were not detected in normal samples and were not found in published SNP databases (dbSNP; http://www.ncbi.nlm.nih.gov/projects/SNP) and/or they were not reported as SNPs in previous publications. Screening for JAK2V617F mutation was performed as previously described.27
Statistics
Demographic and baseline MDS disease characteristics of all patients were summarized descriptively. Severe adverse events and efficacy were summarized for the entire treated population (phase 1 and 2). The safety of the combination was evaluated by the frequency and severity of adverse events according to NCI-CTC Version 3.0 that occurred during the first 4 weeks of therapy and throughout the 7-cycle study period. The incidence and percentage of adverse events were summarized overall and within each dosing cohort. The relationship of baseline erythropoietin levels to response was explored with the Spearman Correlation, logistic regression, and Cox PH survival models.
Objective IWG responses were identified by the investigator at each participating institution, with reports further assessed and confirmed by the primary investigator of the overall study (M.A.S.) and are summarized for the entire cohort by the use of percentages. Categorical variables were analyzed with either χ2 statistics or the Fisher exact test with a 2-sided P value of < .05 considered statistically significant.
Results
Patients
A total of 36 subjects with histologically confirmed MDS were enrolled at the 3 centers, 18 in the phase 1 portion of the study and 18 in the phase 2 continuation (Table 1). The median age was 68 years (range, 47-78 years), and median time from MDS diagnosis was 7 weeks (range, 2-107 weeks). Patients had pancytopenia, with a median blast percentage of 11% (1%-19%). Fourteen patients (39%) had received past red blood cell transfusions at baseline, and 3 patients (8%) had received platelet transfusions. Patients comprised the following WHO classifications: 2 with RA (6%); 3 with chronic myelomonocytic leukemia-2 (8%); 10 with RAEB-1 (28%); and 21 with RAEB-2 (58%), which corresponded to IPSS risk categorizations of intermediate-1 (n = 5, 14%, all with excess blasts); intermediate-2 (n = 20, 56%); and high (n = 11, 31%). Two patients (6%) had a del(5q) cytogenetic abnormality, and 9 patients (25%) had evidence of bone marrow fibrosis. Previous therapies included growth factors (n = 7, 19%), immunosuppressants (n = 5, 14%), or disease-modifying therapies (chemotherapy, n = 6, 17%). Patients received a median of 5 cycles on-study (range, 1-7) and were followed a median of 11.5 months (range, 3-55 months) for all subjects, a median of 12 months (range, 3-52 months) for survivors.
Characteristics of subjects
| Characteristic | Median (range) or N (%) n = 36 |
|---|---|
| Age, y | 68 years (47-78) |
| Female/male, n | 13/23 |
| Time from diagnosis | 7 weeks (2-107) |
| Baseline | |
| Hgb, g/dL | 9.7 (7.1-14.6) |
| Plt, × 103/mL | 65 (3-523) |
| ANC, × 103/mL) | 0.840 (0.24-13.3) |
| Epo, MIU/mL | 108 (17.6-1316.0) |
| Blast % | 11.1 (1-19) |
| IPSS, n | |
| Int-1 | 5 (14) |
| Int-2 | 20 (56) |
| High | 11 (31) |
| IPSS cytogenetics risk group (n = 19), n | |
| Good | 8 (42) |
| Intermediate | 6 (32) |
| Poor | 4 (21) |
| No growth | 1 (5) |
| WHO classification, n | |
| RA | 2 (6) |
| CMML-2 | 3 (8) |
| RAEB-1 | 10 (28) |
| RAEB-2 | 21 (58) |
| Previous therapies, n (%) | |
| Growth factors | 7 (19) |
| Immunosuppressants | 5 (14) |
| Chemotherapy | 6 (17) |
| Median cycles on-study, n (range) | 5 (1-7) |
| Characteristic | Median (range) or N (%) n = 36 |
|---|---|
| Age, y | 68 years (47-78) |
| Female/male, n | 13/23 |
| Time from diagnosis | 7 weeks (2-107) |
| Baseline | |
| Hgb, g/dL | 9.7 (7.1-14.6) |
| Plt, × 103/mL | 65 (3-523) |
| ANC, × 103/mL) | 0.840 (0.24-13.3) |
| Epo, MIU/mL | 108 (17.6-1316.0) |
| Blast % | 11.1 (1-19) |
| IPSS, n | |
| Int-1 | 5 (14) |
| Int-2 | 20 (56) |
| High | 11 (31) |
| IPSS cytogenetics risk group (n = 19), n | |
| Good | 8 (42) |
| Intermediate | 6 (32) |
| Poor | 4 (21) |
| No growth | 1 (5) |
| WHO classification, n | |
| RA | 2 (6) |
| CMML-2 | 3 (8) |
| RAEB-1 | 10 (28) |
| RAEB-2 | 21 (58) |
| Previous therapies, n (%) | |
| Growth factors | 7 (19) |
| Immunosuppressants | 5 (14) |
| Chemotherapy | 6 (17) |
| Median cycles on-study, n (range) | 5 (1-7) |
ANC indicates bsolute neutrophil count; CMML, chronic myelomonocytic leukemia; Epo, erythropoietin level (for all subjects); Hgb, hemoglobin; Int, intermediate; IPSS, International Prognostic Scoring System; Plt, platelet count; RA, refractory anemia; RAEB, refractory anemia with excess blasts; and WHO, World Health Organization.
Assessment of safety
During the first 8 weeks of therapy, the median ANC decrease was 35% (range, 766.2% increase to 100% decrease), and median platelet decrease was 14.6% (range, 344.2% increase to 95.6% decrease). Cycle 2 was delayed in 10 patients for a median of 7.5 days (range, 1-20 days, with 3 patients delayed > 10 days), for recovery of blood counts. Eight subjects had a dose reduction of lenalidomide: 6 were reduced from 10 to 5 mg and completed the study at 5 mg, whereas 2 were reduced to 5 mg and later were increased back to 10 mg. Growth factor support (granulocyte-colony stimulating factor) was allowed per study protocol in the setting of fever and neutropenia or infection and occurred in a total of 19 instances. Grade 3 or 4 nonhematologic toxicities are detailed in Table 2, the most common of which were febrile neutropenia (n = 8, 22%); infection (n = 4, 11%); pulmonary complications (including 1 episode of pneumonitis and 3 of pneumonia, 1 of which was possibly related to therapy; n = 4, 11%); cardiac events (including congestive heart failure, arrhythmia, and a vasovagal episode, all considered unrelated to therapy; n = 4, 11%); constitutional symptoms (n = 4, 11%); and dermatologic (n = 4, 11%), vascular access–related thrombosis, hemorrhage, renal failure, and secondary malignancy affecting 2 patients each (6%). Table 3 contains nonserious, nonhematologic adverse events occurring in > 10% of patients; the most common of these were constipation (56%), fatigue (50%), diarrhea (47%), injection-site reaction (39%), pruritis (28%), dyspnea (28%), rash (25%), nausea (25%), and dizziness (25%). Three patients (8%) died while on study, and 3 (8%) had progressive disease.
Grade 3 or 4 nonhematologic adverse events
| Events | Subjects affected | |
|---|---|---|
| Total n (%) | Treatment-related, n (%) | |
| Febrile neutropenia | 8 (22) | 4 (11) |
| Infection | 4 (11) | 1 (3) |
| Cardiac (arrhythmia, CHF, vasovagal) | 4 (11) | 1 (3) |
| Pulmonary (pneumonitis, pneumonia) | 4 (11) | 1 (3) |
| Constitutional symptoms | 4 (11) | 1 (3) |
| Dermatologic | 4 (11) | 0 (0) |
| Vascular access-related thrombosis | 2 (6) | 0 (0) |
| Hemorrhage | 2 (6) | 0 (0) |
| Renal failure | 2 (6) | 0 (0) |
| Secondary malignancy* | 2 (6) | 0 (0) |
| Other | 4 (11) | 1 (3) |
| Events | Subjects affected | |
|---|---|---|
| Total n (%) | Treatment-related, n (%) | |
| Febrile neutropenia | 8 (22) | 4 (11) |
| Infection | 4 (11) | 1 (3) |
| Cardiac (arrhythmia, CHF, vasovagal) | 4 (11) | 1 (3) |
| Pulmonary (pneumonitis, pneumonia) | 4 (11) | 1 (3) |
| Constitutional symptoms | 4 (11) | 1 (3) |
| Dermatologic | 4 (11) | 0 (0) |
| Vascular access-related thrombosis | 2 (6) | 0 (0) |
| Hemorrhage | 2 (6) | 0 (0) |
| Renal failure | 2 (6) | 0 (0) |
| Secondary malignancy* | 2 (6) | 0 (0) |
| Other | 4 (11) | 1 (3) |
CHF indicates congestive heart failure.
Basal cell carcinoma of the left earlobe and squamous cell carcinoma of the skin.
Nonserious (grade < 2), nonhematologic adverse events affecting > 10% of subjects
| Adverse event | No. (%) subjects affected | No. (%) possibly related to treatment |
|---|---|---|
| Constipation | 20 (55.6) | 14 (70) |
| Diarrhea | 17 (47.2) | 14 (82.4) |
| Injection site reaction | 14 (38.9) | 14 (100) |
| Pruritus | 10 (27.8) | 10 (100) |
| Rash/desquamation | 9 (25) | 9 (100) |
| Fatigue | 18 (50) | 13 (72.2) |
| Nausea | 9 (25) | 8 (88.9) |
| Dizziness | 9 (25) | 3 (33.3) |
| Fever (without neutropenia) | 5 (13.9) | 2 (40) |
| Insomnia | 6 (16.7) | 3 (50) |
| Dyspepsia | 4 (11.1) | 4 (100) |
| Headache | 5 (13.9) | 2 (40) |
| Cough | 8 (22.2) | 0 (0) |
| Dyspnea | 10 (27.8) | 4 (40) |
| Hypotension | 5 (13.9) | 2 (40) |
| Constitutional symptoms, other | 6 (16.7) | 4 (66.7) |
| Rigors/chills | 4 (11.1) | 1 (25) |
| Dermatology/skin, other | 9 (25) | 3 (33.3) |
| Anorexia | 6 (16.7) | 3 (50) |
| Gastrointestinal, other | 4 (11.1) | 1 (25) |
| Dysgeusia | 4 (11.1) | 4 (100) |
| Vomiting | 4 (11.1) | 3 (75) |
| Edema: limb | 5 (13.9) | 2 (40) |
| Adverse event | No. (%) subjects affected | No. (%) possibly related to treatment |
|---|---|---|
| Constipation | 20 (55.6) | 14 (70) |
| Diarrhea | 17 (47.2) | 14 (82.4) |
| Injection site reaction | 14 (38.9) | 14 (100) |
| Pruritus | 10 (27.8) | 10 (100) |
| Rash/desquamation | 9 (25) | 9 (100) |
| Fatigue | 18 (50) | 13 (72.2) |
| Nausea | 9 (25) | 8 (88.9) |
| Dizziness | 9 (25) | 3 (33.3) |
| Fever (without neutropenia) | 5 (13.9) | 2 (40) |
| Insomnia | 6 (16.7) | 3 (50) |
| Dyspepsia | 4 (11.1) | 4 (100) |
| Headache | 5 (13.9) | 2 (40) |
| Cough | 8 (22.2) | 0 (0) |
| Dyspnea | 10 (27.8) | 4 (40) |
| Hypotension | 5 (13.9) | 2 (40) |
| Constitutional symptoms, other | 6 (16.7) | 4 (66.7) |
| Rigors/chills | 4 (11.1) | 1 (25) |
| Dermatology/skin, other | 9 (25) | 3 (33.3) |
| Anorexia | 6 (16.7) | 3 (50) |
| Gastrointestinal, other | 4 (11.1) | 1 (25) |
| Dysgeusia | 4 (11.1) | 4 (100) |
| Vomiting | 4 (11.1) | 3 (75) |
| Edema: limb | 5 (13.9) | 2 (40) |
Assessment of efficacy
All patients were evaluable for efficacy. Among 36 subjects, 26 (72%) responded to therapy: 16 achieved a CR (44%) and 10 a hematologic improvement (28%), of whom 10 of the CR patients also had a bi- or trilineage hematologic response (Table 4). Initial responses occurred a median of 3.7 months (range, 1.4-7.4 months) after the start of therapy and were sustained in patients with CR for a median of 17+ months (range, 3-39+ months).
Efficacy of combination azacitidine and lenalidomide
| Characteristic | n (% or range) |
|---|---|
| Overall response rate | 26/36 (72) |
| CR | 16 (44) |
| HI | 10 (28) |
| HI, erythroid | 3 (30) |
| HI, platelet | 3 (30) |
| HI, neutrophil | 4 (40) |
| Median time to initial response, mo | 3.7 (1.4-7.4) |
| Median CR duration, mo | 17+ (3-39+) |
| Median overall survival, mo, n = 36 | 13.6 (3-55) |
| Median overall survival among CR patients, mo, n = 16 | 37+ (7-55+) |
| Characteristic | n (% or range) |
|---|---|
| Overall response rate | 26/36 (72) |
| CR | 16 (44) |
| HI | 10 (28) |
| HI, erythroid | 3 (30) |
| HI, platelet | 3 (30) |
| HI, neutrophil | 4 (40) |
| Median time to initial response, mo | 3.7 (1.4-7.4) |
| Median CR duration, mo | 17+ (3-39+) |
| Median overall survival, mo, n = 36 | 13.6 (3-55) |
| Median overall survival among CR patients, mo, n = 16 | 37+ (7-55+) |
CR indicates complete response; and HI, hematologic improvement.
Of those who achieved CR, the median age was 69 years, and patients comprised the following WHO/IPSS categories, respectively: RA (n = 1, 6%), RAEB-1 (n = 8, 50%), RAEB-2 (n = 7, 44%), intermediate-1 (n = 4, 25%), intermediate-2 (n = 10, 63%), and high (n = 2, 13%). Baseline erythropoietin levels were not significantly related to achievement of a CR (Spearman correlation coefficient = −0.145, P = .4366; Logistic regression parameter estimate −0.00039, P = .721; Cox PH model parameter estimate −0.00061, P = .446). Among patients with CR, 6 of 16 (38%) had already received red blood cell transfusions at the time of study enrollment, compared with 8 of 20 (40%) of those who did not achieve a CR (P = .879); 1 of 16 (6%) of those who achieved CR had already received platelet transfusions at baseline, versus 2 of 20 (10%) of those who did not achieve a CR (P = .686).
A red blood cell and platelet transfusion rate was calculated by totaling the number of transfusions received, respectively, and dividing by the number of months of follow-up. Comparing the rates for those achieved a CR versus those who did not, we found that the red blood cell transfusion rates were 0.20 per month versus 1.23 per month, respectively (P = .0023), whereas platelet transfusion rates were 0.92 per month versus 0.17 per month, respectively (P = .0216). Eight patients with CR (50%) evolved to AML a median of 18 months after achieving CR (range, 6-26 months); one subsequently died in CR, one had a last known status of hematologic improvement and subsequently died, and 6 were alive at the last study assessment. All responding patients remained on combination therapy for the first 7 cycles, and azacitidine monotherapy thereafter, until loss of response or death. The median OS was 13.6 months for the entire cohort (range, 3-55 months), and 37+ months for patients achieving CR (range, 7-55+ months).
Metaphase karyotyping, SNP-A karyotyping, and mutational analyses
Cytogenetics subgroups among patients with CR included normal (n = 9, 64%), del(5q) (n = 2, 14%), +8 (n = 1, 7%), complex (n = 1, 7%), and unknown (n = 1, 7%). Nineteen patients (63%) had metaphase karyotyping results available before and after therapy (Table 5, supplemental Tables 1 and 2, available on the Blood Web site; see the Supplemental Materials link at the top of the online article). Among 19 of these patients who had an IWG response, no patients who started with normal cytogenetics had cytogenetic evolution, whereas of the 10 patients with abnormal baseline cytogenetics, 3 (30%) normalized their karyotype, all of whom achieved CR. For 14 patients, both metaphase cytogenetics and SNP-A–based karyotyping were available (Table 5). Of 10 patients with baseline new or additional SNP-A lesions present, 4 had gains, 4 had losses, and 2 had both gains and losses, of whom one also had uniparental disomy. Only 2 of these patients had normal metaphase cytogenetics. The majority of patients who had good and intermediate-risk karyotype by IPSS cytogenetic risk grouping achieved CR (93%). Among the 10 patients with additional or new SNP-A lesions identified, 8 (80%) achieved a CR or HI, compared with 3 patients (75%) without new or additional SNP lesions. Among these 19 patients, none with complex karyotype, defined as the presence of ≥ 3 chromosomal abnormalities at initial presentation, responded.
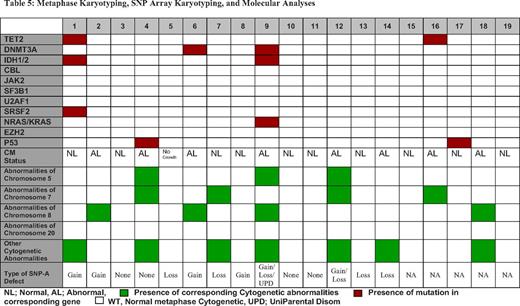
Of 19 patients who underwent molecular mutational analysis, 6 had specific molecular abnormalities: 1 with TET2, IDH1/2, and SRSF2 mutations, 1 with TET2, IDH1/2, and KRAS mutations, 1 with a DNMT3A mutation, 2 with sole p53 mutations, and 1 with an isolated TET2 mutation (supplemental Table 1). Five of 6 (83%) achieved a CR compared with 46% of those who were wild type for these abnormalities (P = .12). One patient who harbored a p53 mutation but had a complex karyotype at initial presentation did not respond to therapy. All patients were negative for CBL, JAK2V617F, U2AF1, NRAS, EZH2, and SF3B1 mutations. All patients who carried a TET2, IDH1/2, or DNMT3A mutation achieved a CR.
Discussion
The phase 1 combination trial of lenalidomide and azacitidine was the first to combine 2 drugs approved by the US Food and Drug Administration specifically for the treatment of MDS, thereby establishing tolerable therapeutic drug doses and schedules.20 The justification for this strategy rested in the theory that patients with higher-risk MDS also retained properties of the lower-risk MDS from which their disease likely evolved and that the use of 2 agents with complementary mechanisms of action may yield synergistic benefit. In this study, median neutrophil and platelet decrease was approximately 25%; severe (grade 3 or 4) nonhematologic toxicities were comparable with those seen with the individual agents; and the overall response rate was 67%, including a CR rate of 44%. This multi-institution, phase 2 expansion study verifies the safety and efficacy of the combination observed in the initial trial, provides long-term follow-up of responding patients from both study phases along with more extensive adverse event reporting, and suggests a molecularly favorable group.
Five-day azacitidine dosing was determined on the basis of a prospective study in community oncology groups examining azacitidine administered in a 5-2-2 schedule (75 mg/m2/d subcutaneously for 5 days, followed by 2 days no treatment, then 75 mg/m2/d for 2 days); in a 5-2-5 schedule (50 mg/m2/d subcutaneously for 5 days, followed by 2 days no treatment, then 50 mg/m2/d for 5 days); or in a 5-day schedule (75 mg/m2/d subcutaneously for 5 days).28 There were no differences in response rates for any schedule when both lower- and higher-risk patients with MDS were treated. Another US prospective, longitudinal, multicenter registry study collected data on 380 patients with MDS who were treated with azacitidine. In exploring dosing schedules, the authors again found no differences in responses for 7-day continuous dosing; 7-day interrupted dosing (such as the 5-2-2 schedule); and for < 7-day dosing.29 Lenalidomide dosing was determined by the schedules used in phase 1/2/3 prospective studies in patients with MDS, with escalation to the single-agent therapeutic dose of 10 mg daily.19,30
An initial concern in combining these drugs was the risk of added toxicity with 2 myelosuppressive agents. The median decreases in neutrophil and platelet counts, however, were mild at 35% and 15%, respectively, and self-limited in responding patients. We used functional definitions of relative neutrophil and platelet decrements, rather than absolute CTC criteria, so as to avoid attributing treatment-related myelosuppression to a patient entering the study with significant baseline cytopenias, and limited assessment to the first 8 weeks of therapy, so as not to confound the assessment with cytopenias attributable to disease progression.31 Other serious adverse events occurred with a similar frequency to that seen with either monotherapy in a similar, greater-risk MDS population.23,32
The combination of lenalidomide and azacitidine was highly effective, with an overall response rate of 72%, and a high CR rate of 44%, in comparison with the overall response rate of 49%, which included a CR rate of 17%, seen in the phase 3 AZA-001 study for higher-risk MDS patients randomized to receive azacitidine.23 One possible contributing factor to these discrepancies in response rate could be the inclusion of some intermediate-1 patients in the present study (albeit, all with excess blasts), with a resultant lower percentage of IPSS high-risk patients compared with AZA-001 (31% vs 46%, respectively). Response rates seen in this combination study are superior to those seen in lower-risk MDS patients without the del(5q) cytogenetic abnormality treated with lenalidomide13 and to those reported in lenalidomide-treated, higher-risk del (5q) MDS and patients with AML.16,32
The median OS for the entire population was shorter than in the AZA-001 study, at 13.6 months compared with 24.5 months, which likely reflects shorter median follow-up (11.5 months vs 21.1 months), different patient populations, and that survival was a secondary objective in the current study. Despite this, median OS for patients with CR exceeded 3 years. The synergistic activity of the azacitidine + lenalidomide combination is further supported by a follow-up report of the phase 1 combination trial, in which 3 patients who achieved a CR within the 7-cycle combination therapy time period then continued on azacitidine monotherapy for an additional 12-24 months before relapsing with cytopenias and excess blasts. They all regained their CR status solely with the reinitiation of lenalidomide combined with their on-going azacitidine therapy, demonstrating additional benefit of the combination, with each patient serving as his own control.33 Given lenalidomide's particular action on erythroid improvement in lower-risk populations, it is possible that it contributed to greater erythroid responses in this higher-risk population, which in turn could have contributed to a greater CR rate.
We also performed a comprehensive cytogenetic and molecular analysis of subjects. Patients with IPSS good- and intermediate-risk cytogenetic abnormalities achieved high CR rates. Patients with lesions identified by SNP arrays before therapy had greater rates of CR, whereas those with complex karyotype as determined by metaphase cytogenetics before initiating treatment were less likely to respond. Patients who had molecular abnormalities along a methylation pathway, including TET2, DNMT3A, and IDH 1/2, even in the presence of additional molecular mutations typically associated with poor outcomes in MDS (patients 4 and 9), appeared more likely to achieve a CR to combination therapy (83% of affected patients), compared with less than half the patients who did not harbor one of these lesions, although limited samples prevented this finding from reaching statistical significance. This result supports the findings of recent studies in which investigators showed that the presence of specific molecular mutations involving the epigenetic machinery, specifically TET2, are predictive of better response to hypomethylating agents.34-36 Although intriguing, because of the heterogeneity of the population and small sample size, these results remain to be validated in larger treated cohorts.
The azacitidine + lenalidomide combination has been explored in a preliminary fashion in other MDS and AML populations. One phase 1 study of the combination administered sequentially reported a CR/incomplete CR rate of 44% in previously untreated, older AML patients,37 whereas other studies are exploring the combination in the same population with lenalidomide administered at 50 mg daily and increasing doses of concomitant azacitidine (NCT1016600); sequentially in relapsed/refractory AML or higher-risk MDS with chromosome 5 abnormalities (NCT00923234); and sequentially in relapsed/refractory AML or MDS of any age or untreated older adults with AML or MDS (NCT01038635). It remains to be seen whether continuing the combination beyond 7 cycles can yield more durable responses; whether this regimen would be more tolerable with better efficacy if administered sequentially; and whether it would be more ideally suited for higher-risk MDS patients with the del (5q) cytogenetic abnormality because this cohort included only 2 such patients (both of whom attained a CR). The azacitidine + lenalidomide combination is being compared with azacitidine monotherapy, as is azacitidine + vorinostat (a histone deacetylase inhibitor), in a North American Intergroup protocol (S1117, NCT01522976).
In conclusion, the combination of lenalidomide and azacitidine is well-tolerated and highly effective in higher-risk MDS patients, with sustained responses seen. Patients with molecular abnormalities along the methylation pathway appear more likely to achieve a CR.
There is an Inside Blood commentary on this article in this issue.
The online version of this article contains a data supplement.
Presented in part at annual meetings of the American Society of Hematology in Atlanta, GA on December 9, 2007; in San Francisco, CA on December 6, 2008; and in San Diego, CA on December 12, 2011, and published in abstract form.38
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This research was supported, in part, by National Institutes of Health U54RR19397-03 (to M.A.S., A.F.L., R.P., and J.P.M.), Cleveland Clinic Seed Support, and an MDS Foundation grant (R.V.T.).
National Institutes of Health
Authorship
Contribution: M.A.S. designed and performed the research, analyzed the data, and wrote the manuscript; R.V.T. performed the research, analyzed the data, and wrote the manuscript; R.K., J.L., A.S.A., M.A., R.E., J.J., J.P., and R.P. performed the research and edited the manuscript; A.F.L. designed and performed the research and edited the manuscript; D.C. analyzed the data; A.T., V.V., H.M., and A.J. performed the research and edited the manuscript; and J.P.M. designed and performed the research, analyzed the data, and wrote the manuscript.
Conflict-of-interest disclosure: M.A.S. has received consulting fees and is on an advisory board for Celgene Corp and Amgen. R.V.T., R.K., A.F.L., and J.P.M. have served on advisory boards for Celgene Corp. The remaining authors declare no competing financial interests.
Correspondence: Mikkael A. Sekeres, MD, MS, Associate Professor of Medicine, Director, Leukemia Program, Department of Hematologic Oncology and Blood Disorders, Cleveland Clinic Taussig Cancer Institute, Desk R35, 9500 Euclid Ave, Cleveland, OH 44195; e-mail: sekerem@ccf.org.
