Key Points
PTCY results in a lower incidence of severe acute GVHD compared with ATG in patients transplanted from 9/10 MMUD for acute myeloid leukemia.
PTCY results in better survival compared with ATG in patients transplanted from 9/10 MMUD for acute myeloid leukemia.

Abstract
The use of anti-thymocyte globulin (ATG) has represented the standard of care in graft-versus-host disease (GVHD) prophylaxis in patients undergoing a mismatched unrelated donor (MMUD) transplant. The safety and feasibility of posttransplant cyclophosphamide (PTCY) in this setting have been reported recently, but no study has compared the outcomes of PTCY vs ATG in 9/10 MMUD transplants. Using the registry data of the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation, we performed a matched-pair analysis comparing those 2 strategies in a 9/10 MMUD setting. Ninety-three patients receiving PTCY were matched with 179 patients receiving ATG. A significantly lower incidence of severe acute GVHD was observed with PTCY compared with ATG. Recipients of the former also showed higher leukemia-free survival and GVHD/relapse-free survival (GRFS). When performing a subgroup analysis including patients receiving peripheral blood stem cells, being in complete remission, or receiving the same associated immunosuppressive agents, superiority of PTCY over ATG was confirmed. Similar to the haploidentical setting, use of PTCY is an effective anti-GVHD prophylaxis in the 9/10 MMUD transplant. Use of PTCY may also provide better outcomes in long-term disease control. These results need confirmation in large prospective randomized trials.
Introduction
In patients lacking an HLA-identical sibling or unrelated donor (UD), several options exist, including haploidentical donors, mismatched unrelated donors (MMUDs), and unrelated cord blood units. However, the existence of HLA mismatches has historically been associated with worse overall outcomes, particularly in terms of graft-versus-host disease (GVHD) and nonrelapse mortality (NRM).1-5 Subsequently, strategies aiming to improve GVHD prophylaxis to overcome the HLA barrier have been introduced.6,7 The use of in vivo T-cell depletion (TCD) with anti-thymocyte globulin (ATG) or alemtuzumab, in association with a calcineurin inhibitor and methotrexate or mycophenolate mofetil, has represented the standard of care in the presence of HLA mismatches.8 More recently, the Johns Hopkins group pioneered the use of posttransplant cyclophosphamide (PTCY) in the haploidentical donor setting, with significant improvements in the rates of GVHD, NRM, and engraftment.9 Since then, PTCY has been applied in other settings, including HLA-identical sibling or UD and MMUD.10-13 Although reports on the use of PTCY exist in the HLA-identical setting, only 2 single-center studies have compared the outcomes of patients undergoing an MMUD transplant with PTCY or ATG as GVHD prophylaxis in small cohorts. Moreover, in those series, the study population was heterogeneous and included different hematological diseases.14,15
In the current study, we retrospectively analyzed results of allogeneic hematopoietic stem cell transplantation (allo-HSCT) from MMUDs in a homogenous population of acute myeloid leukemia (AML) patients, comparing the outcomes of PTCY vs ATG as GVHD prophylaxis.
Methods
This is a retrospective study from the European Society for Blood and Marrow Transplantation (EBMT) Acute Leukemia Working Party (ALWP), which is a working group of >600 transplant centers, primarily located in Europe, that are required to report all consecutive transplantations and follow-up data annually (supplemental Materials, available on the Blood Web site). Data are entered, managed, and maintained in a central database with Internet access; each EBMT center is represented in this database. There are no restrictions on centers for reporting data, except for those required by law on patient consent, data confidentiality, and accuracy. Quality-control measures include several independent systems: confirmation of validity of the entered data by the reporting team, selective comparison of the survey data with MED-A data sets in the EBMT registry database, cross-checking with the national registries, and regular in-house and external data audits. Patients provide informed consent authorizing the use of their personal information for research purposes. Each patient provides consent for transplant according to the Declaration of Helsinki.
The study was approved by the Institutional Review Board of the ALWP of the EBMT.
Eligibility criteria
Included in the current study were adult patients (age ≥ 18 years) diagnosed with AML and undergoing their first allo-HSCT from a 9/10 MMUD during the period from 2011 to 2017. Only cases for whom high-resolution HLA allele typing at loci A, B, C, DRB1, and DQ was available in the EBMT registry for the patient and the donor were included. A 9/10 MMUD was defined as the presence of a mismatch at 1 of the aforementioned loci.
Among patients undergoing allo-HSCT from 9/10 MMUDs, only those for whom GVHD prophylaxis contained PTCY or ATG were included. In vivo TCD other than ATG was excluded.
Patients being either in complete remission (CR) or transplanted with active disease at time of allo-HSCT were included. The cytogenetic risk was defined according to Grimwade et al.16 Performance status was graded according to the Karnofsky Performance Status and was defined as poor when <90. Conditioning regimen was defined, based on data reported by the centers, as myeloablative conditioning (MAC) or reduced-intensity conditioning (RIC), according to EBMT definition.17
The primary end point of the study was the cumulative incidence of GVHD. Acute GVHD (aGVHD) was graded according to the modified Glucksberg criteria,18 and chronic GVHD (cGVHD) was graded based on the revised Seattle criteria.19 Secondary end points included engraftment rate, leukemia-free survival (LFS), overall survival (OS), refined GVHD/relapse-free survival (GRFS), cumulative incidence of relapse (RI), and NRM.
Engraftment was defined as achieving an absolute neutrophil count ≥ 0.5 × 109/L for 3 consecutive days. LFS was defined as the probability of being alive without evidence of relapse or progression. OS was defined as the time from allo-HSCT to death, regardless of the cause. Refined GRFS was defined according to Ruggeri et al (ie, being alive with no grade III-IV aGVHD, severe cGVHD, or disease relapse at any time point).20 Relapse was defined as the presence of 5% bone marrow blasts and/or reappearance of the underlying disease. NRM was defined as death without evidence of relapse or progression.
Statistical methods
Patient-, disease-, and transplant-related characteristics were compared using the χ2 or Fisher’s exact test for categorical variables, and the Mann-Whitney U test was used for continuous variables. Probabilities of OS, LFS, and GRFS were calculated using the Kaplan-Meier method.21 Cumulative incidence functions (CIFs) were used to estimate RI and NRM in a competing risk setting. To study GVHD, death and relapse were considered competing events. Univariate analyses were performed using the log-rank test for OS, LFS, and GRFS, whereas Gray’s test was used for CIFs.22 Propensity score matching was also performed to reduce or eliminate confounding effects. Each identified patient who received PTCY was matched with 2 patients who received ATG. Matching was done without replacement. Exact matching was used for disease status at transplant and conditioning intensity, nearest matching neighbor for age, source of stem cells, secondary AML, patient and donor cytomegalovirus (CMV) serology status, and female donor/male recipient. Matching was done on the logit of the propensity score using calipers with a width equal to 0.2 of the standard deviation of the logit of the estimated propensity score.23 This caliper width has been found to result in optimal estimation of risk differences in a variety of settings.24 All tests were 2-sided, and P < .05 was considered statistically significant. Analyses were performed using R statistical software version 3.2.3 (http://www.R-project.org), and propensity score matching was performed using the MatchIt package (https://cran.r-project.org/web/packages/MatchIt/MatchIt.pdf).
Results
The baseline characteristics are summarized in Table 1. Globally, 1001 and 102 patients receiving ATG or PTCY, respectively, who fulfilled the inclusion criteria were identified. Among patients receiving PTCY, we excluded 9 from the analysis because of the absence of a corresponding match with the ATG group (n = 4) or missing data for the pair matching (n = 5). Subsequently, we were able to match 93 patients receiving PTCY to 179 receiving ATG. The median age at transplant was 53 years (range, 19-75) and 51 years (range, 20-73) in the ATG and PTCY groups, respectively (P = .98). A higher proportion of female patients was observed in the PTCY group (60% vs 45% in the ATG group, P < .02). Female donors/male recipients were observed in 10% of cases. Of note, HLA class I mismatches were the most frequently observed in the ATG (75%) and PTCY (73%) groups. At the time of allo-HSCT, nearly 55% of patients were in first complete remission (CR1) and 16% were in CR2 or beyond in both groups. Active disease was observed in nearly 28% of patients. An interval of 6 months from diagnosis to transplant was observed in both groups. Patients receiving ATG were transplanted earlier, primarily in 2014 (range, 2011-2017) compared with patients receiving PTCY, who were primarily transplanted in 2015 (range, 2011-2017) (P < .01). This translated into a longer median follow-up for the ATG group (27 months [range, 2-83] vs 14 months [range, 2-56] in the PTCY group [P < .01]). The median dose of ATG changed according to the brand used: 6 mg/kg (range, 2.5-15) for thymoglobulin and 30 mg/kg (range, 17-60) for Fresenius. Peripheral blood stem cells were the most frequently used stem cell source (91% in both groups). No differences in terms of graft composition were observed in the 2 groups. Patients with a positive CMV serology were transplanted from seronegative donors in 38% of cases in the ATG group and in 30% of cases in the PTCY group. The 2 cohorts were equally distributed among MAC and RIC conditioning regimens. A busulfan and fludarabine–based regimen was the most frequently used conditioning in the PTCY group (MAC and RIC) and in the ATG group (only RIC). Busulfan and cyclophosphamide was the most frequently used MAC in the ATG group.
Cyclosporine and mycophenolate mofetil were the most frequent immunosuppressive agents associated with GVHD prophylaxis in the PTCY (42%) and ATG (49%) groups, followed by cyclosporine and methotrexate (39%) and tacrolimus and mycophenolate mofetil (20%) in the ATG and PTCY groups, respectively.
Engraftment
The engraftment rate was similar in both groups: 96% and 95% in the ATG and PTCY groups, respectively (P = .7); however, the median time to neutrophil engraftment was shorter in the ATG group (17 days vs 19 days in the PTCY group, P < .01). Globally, 37 and 4 patients in the ATG and PTCY groups, respectively, experienced graft failure.
Survival outcomes
aGVHD and cGVHD
The cumulative incidence of grade II-IV aGVHD at 100 days was similar between the 2 groups: 30% in patients receiving PTCY compared with 32% in the ATG group (P = .39). Furthermore, use of PTCY was associated with a significantly lower incidence of grade III-IV aGVHD (9% vs 19% in the ATG group, P < .04). At 2 years, no difference in the cumulative incidence of cGVHD of any grade, including extensive cGVHD, was found between the PTCY and ATG groups.
Other survival outcomes
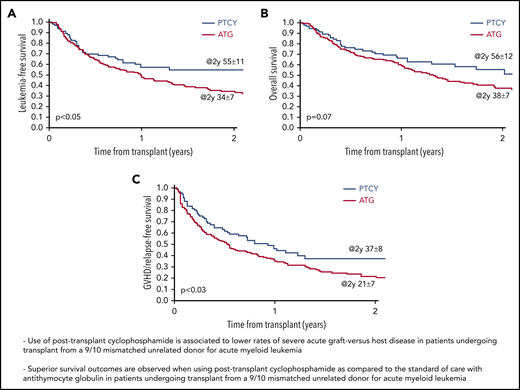
Interestingly, patients who received PTCY experienced a significantly higher probability of LFS (55% vs 34% for patients receiving ATG, P < .05). Similarly, a trend for a higher probability of OS was observed in the PTCY group (56%) compared with the ATG group (38%) (P < .07) (Figure 1A-B). A significantly higher probability of GRFS at 2 years was observed in the PTCY group (37% vs 21% in the ATG group, P < .03) (Figure 1C). No differences in terms of RI or NRM were found based on the GVHD prophylaxis strategy used (Figure 2). Death was primarily attributable to disease recurrence (40% vs 37%), followed by infections (25% vs 20%) and GVHD (24% vs 9%), in the ATG and PTCY groups, respectively.
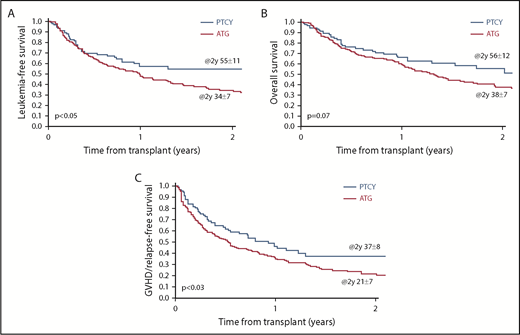
Results of pair-matched analysis for 2 years LFS, OS, and GVHD/GRFS. LFS (A), OS (B), and GRFS (C).
Results of pair-matched analysis for 2 years LFS, OS, and GVHD/GRFS. LFS (A), OS (B), and GRFS (C).
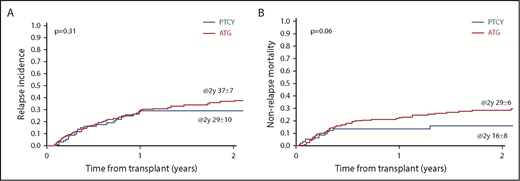
Results of matched-pair analysis for 2-year cumulative incidence of RI and NRM. RI (A) and NRM (B).
Results of matched-pair analysis for 2-year cumulative incidence of RI and NRM. RI (A) and NRM (B).
Subgroup analysis in patients receiving cyclosporine and mycophenolate mofetil
We subsequently restricted our matched-pair analysis to 3 subgroups: (1) patients receiving cyclosporine and mycophenolate mofetil (most popular associated immunosuppressive agents in both groups) as GVHD prophylaxis in association with PTCY (n = 38) or ATG (n = 87), (2) patients in CR at the time of allo-HSCT, and (3) patients receiving PBSCs as stem cell source (representing >90% of patients in both groups).
Globally, these subgroup analyses confirmed the results for the entire population, showing even better OS in the PTCY group for patients undergoing allo-HSCT in CR or receiving PBSCs and lower NRM in the PTCY group with the use of PBSCs (Tables 4 and 5). Of note, similar results were obtained when excluding patients transplanted in the presence of a DQ mismatch (data not shown).
Discussion
Despite the widespread use of haploidentical donor transplants in recent years, there is still a proportion of patients for whom the only available option is to undergo a 9/10 MMUD allo-HSCT.25 Similar to the haploidentical donor setting, the existence of HLA mismatches in 9/10 MMUD recipients prompts the intensification of GVHD prophylaxis to overcome the HLA barrier; however, there is no consensus about the best strategy for GVHD prophylaxis in this setting.
Furthermore, regardless of donor type, other factors, such as stem cell source, donor and patient CMV serology, and donor and patient gender, are known to significantly influence the occurrence of GVHD and, therefore, must be taken into account when analyzing patient outcomes.26-28
Therefore, in the current study, we compared 2 GVHD prophylaxis strategies, ATG and PTCY, in the setting of a 9/10 MMUD transplant. To eliminate confounding factors and to balance the 2 groups, we performed a matched-pair analysis, taking into account factors mainly influencing GVHD, thus allowing the identification of 93 patients receiving PTCY matched to 179 patients receiving ATG.
Use of ATG has historically represented the standard of care in this setting, because it is capable of partially overcoming the HLA barrier; however, its use has been tainted by concerns primarily related to the risk of infections, delayed immune reconstitution, and relapse.6,29 More recently, the introduction of PTCY in the haploidentical donor setting, prompting selective in vivo allodepletion, allowed for promising results in terms of reduced NRM due to fewer GVHD and infectious morbidities.9 Multiple reports have confirmed its feasibility and efficacy, with similar survival outcomes when PTCY haploidentical donor transplants were compared with other donor sources in different hematological diseases.30-32 Subsequently, several studies also investigated the use of PTCY in the setting of matched sibling donors or UDs and, again, supported its value.10-12
In particular, the Johns Hopkins group reported the efficacy and feasibility of using PTCY alone in patients undergoing HLA-identical UD transplantation with bone marrow as the stem cell source.33 On the other hand, PTCY alone in the same donor setting, with PBSCs as the stem cell source, resulted in unacceptable rates of severe GVHD, prompting the belief that additional prophylactic agents are recommended when using PBSCs.34,35 Mielcarek et al reported that PTCY + cyclosporine A started on day 5 after allo-HSCT resulted in a low incidence of severe aGVHD; however, grade II-IV aGVHD and extensive cGVHD reached 77% and 30%, respectively.10 In another study, the use of PTCY combined with other agents, such as tacrolimus or mycophenolate mofetil, was shown to reduce the incidence of aGVHD and cGVHD to 17% and 7%, respectively, in PBSC recipients.11
In our cohort, we showed significantly lower rates of grade III-IV aGVHD and similar rates of grade II-IV aGVHD and any grade of cGVHD with the use of PTCY compared with ATG. Furthermore, we also observed significantly superior survival outcomes in terms of LFS and GRFS with the use of PTCY.
Of note, nearly 90% of patients in both groups received a PBSC graft. Interestingly, when limiting our analysis to patients receiving PBSC grafts, we found similar results in terms of severe GVHD, LFS, and GRFS and observed significantly higher OS and lower NRM in the PTCY group.
All patients received PTCY or ATG in association with 1 or 2 immunosuppressive agents. To date, the question about the best combination remains unanswered with differences related to center policies still being important, as reflected by our multicenter study. Despite the unbalanced distribution of immunosuppressive agents associated with ATG or PTCY, we performed a subgroup analysis for those patients receiving the same associated immunosuppressive agents (ie, cyclosporine A + mycophenolate mofetil) and found similar results compared with those from the entire population. When limiting our analysis to patients being in CR at the time of allo-HSCT, our results were also confirmed.
Our results for aGVHD are, in part, in line with a single-center study comparing PTCY and ATG in 9/10 MMUD transplants, showing a lower rate of aGVHD in the PTCY group. In that cohort, no differences were found for the other outcomes because of the low number of patients associated with a single-center experience.14 However, the results from that study corroborate the hypothesis that PTCY is safe and produces similar results to conventional GVHD prophylaxis in the setting of 9/10 MMUD transplants.
Our outcomes are also consistent with a single-center experience reported by Jorge et al, showing similar rates of grade II-IV (31%) and grade III-IV aGVHD (8%) in 9/10 MMUD recipients diagnosed with different hematologic malignancies.12
Kasamon et al also reported favorable results in a small group of patients receiving a nonmyeloablative regimen followed by the use of PTCY and mycophenolate mofetil + sirolimus in the setting of 9/10 MMUD transplants, as well as in cases with >1 antigen mismatch, showing low incidences of aGVHD and cGVHD and an NRM of 6% at 2 years.36
We also found results similar to those of Soltermann et al, who compared lower doses of PTCY (40 mg/kg) with ATG and found significantly lower rates of grade II-IV GVHD and higher OS when using PTCY. On the other hand, they did not find any difference in terms of LFS.15
Overall, our findings emphasize that PTCY represents a valid and safe strategy for preventing severe aGVHD, in line with results reported in the haploidentical donor setting.9 It has been widely reported that the efficacy and safety of PTCY are related to a selective depletion of alloreactive T cells, without cytotoxic effects on donor hematopoietic stem cells, thus reducing the incidence of GVHD.37
In our series, the differences in OS and NRM between the 2 groups may be explained, in part, by the higher mortality due to infections and GVHD in the ATG group and higher LFS in the PTCY group, both resulting in higher OS in the PTCY group. Unfortunately, we do not have data on infectious complications in the 2 groups because of the inherent limits of a registry retrospective analysis.
Previously, our group compared PTCY and ATG in the haploidentical donor setting and found the same results, with more favorable outcomes in patients receiving PTCY.38 The latter results highlight that the historical concept of donor immune-mediated antileukemic effects developing in parallel with GVHD, better known as the graft-versus-leukemia effect, is probably not the only mechanism that protects from disease relapse when using PTCY. The former may well provide a direct immune-mediated specific antileukemic effect, distinct from GVHD, that is probably mediated by release of cytokines or other molecules to which leukemic cells may be more sensitive than normal cells. Regardless of the mechanism of action, cells mediating an antileukemic effect seem relatively resistant to PTCY, thus providing a possible explanation for the long-term disease control in the absence of GVHD. However, there are likely other factors that explain the higher LFS with the use of PTCY in our cohort. Unfortunately, we do not have details about disease biology at time of diagnosis, which may have played a role.
On the other hand, the similar incidence of cGVHD with ATG or PTCY may be due to the ability of ATG to reduce the risk of cGVHD, as previously reported.39,40 This was primarily explained by the mechanism of action of ATG, which acts with an extensive in vivo TCD and expansion of regulatory T cells, as well as by targeting B cells. Considering that donor T and B cells play an essential role in the development of cGVHD, the long-term inhibitory action of ATG on these cells may help to prevent this complication.41,42
We acknowledge important limitations of our study, mainly related to its retrospective nature, including the short median follow-up of 14 months for the PTCY group and the lack of aforementioned data (eg, infections, disease biology). However, this is the largest reported series to date providing proof of the superiority of PTCY over ATG in preventing severe GVHD, as well as favoring better long-term survival with long-term disease control.
These results may pave the way to the future use of PTCY as standard of care in this setting of patients; however, larger and prospective series are warranted to confirm our results.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgment
The authors thank Emmanuelle Polge from the ALWP office, EBMT.
Authorship
Contribution: G.B. and M.L. designed the study; M.L. performed the statistical analyses; G.B. wrote the manuscript; A.R., A.N., and M.M. revised the manuscript; N.K., A.V., B.A., I.H., J.S., A.G., D.B., M.I.-R., J.R.P., F.B., and J.F. were the principal investigators at the centers recruiting the largest numbers of patients for the study; and all authors reviewed the final version of the manuscript.
Conflict-of-interest disclosures: F.B. has served on the advisory board for and received speakers’ fees from NEOVII. J.F. has received research grants and speakers’ honoraria from NEOVII. The remaining authors declare no competing financial interests.
Correspondence: Giorgia Battipaglia, Service d’Hématologie clinique et de Thérapie cellulaire, Assistance Publique-Hôpitaux de Paris, Hôpital Saint-Antoine, 184 rue du Faubourg Saint Antoine, 75012 Paris, France; e-mail: giorgicchia@gmail.com.