

Key Points
Clinical, research and mentorship experiences in hematology are positively associated with fellows' plans to pursue hematology-only careers.

Abstract
As the adult hematology and oncology fellowship training pathways have merged in the United States and concerns have arisen about the aging of practicing hematologists, the American Society of Hematology and hematology education leaders are looking to improve their understanding of the factors that contribute to fellows’ plans to enter hematology-only careers. With the support of the American Society of Hematology, we collected and analyzed data from a survey of hematology/oncology fellows (n = 626) to examine the relationship between training and mentorship experiences and fellows’ plans to enter hematology-only careers. Fellows who planned to enter hematology-only careers were significantly more likely to report having clinical training and mentorship experiences in hematology throughout their training relative to fellows with oncology-only or combined hematology/oncology career plans. After controlling for prior interest in hematology and demographic characteristics, exposure to hematology patients in medical school and fellowship, hematology research experiences, and hematology mentorship (research collaboration and career coaching) were positively and significantly associated with hematology-only career plans. These findings suggest that increasing opportunities for exposure to hematology patients, research opportunities and mentors throughout training could be helpful in building a strong pipeline of potential hematologists.
Introduction
Continuous and rapid changes to health care delivery, growing demand for specialty care, and new career options for physicians have created an increased interest among medical specialty societies and practitioners in understanding the factors that influence trainees’ specialty and career choices.1-3 This interest is particularly acute in the hematology community given that over the past 25 years its fellowship training pipeline has become almost entirely integrated with oncology. When the Accreditation Council for Graduate Medical Education (ACGME) began accrediting combined hematology/oncology fellowship programs in 1995, training programs for hematology and oncology were evenly distributed among hematology only (74 programs), combined hematology/oncology (75 programs), and oncology only (83 programs; ACGME).4 By 2018, only 2 single-specialty adult hematology programs remained, along with 146 combined hematology/oncology programs and 7 single-specialty oncology programs.5,6
Adult hematology/oncology fellowships remain relatively competitive compared with other specialties, with few unfilled slots in recent match cycles. In 2018, more than 60% of adult hematology/oncology fellowship positions offered were filled by US graduates and 99% were filled overall.7 Despite these indicators that hematology/oncology fellowships are attractive to trainees in general, that nearly all future hematologists train in combined fellowship programs has caused concern in the hematology community that hematology/oncology fellows do not receive adequate preparation and exposure to hematology patients to motivate them to choose careers in hematology.8,9 Further, some observers have suggested that declines in National Institutes of Health funding for new investigators may discourage aspiring physician-scientists from pursuing careers in fields such as hematology that place a strong emphasis on academic practice and research grant funding.10 These concerns about whether fellows will pursue hematology are particularly acute given perceptions that the specialty is likely to lose many practicing hematologists to retirement, whereas the demand for hematology services continues to increase.11
Given the wide range of career options available to graduates of hematology/oncology fellowship programs, including benign hematology, malignant hematology, solid tumor oncology and careers that combine 2 or more subfields, it is vital to understand fellows’ career choices (and the factors that influence them) to better anticipate future hematology workforce needs. A single-institution survey found that hematology/oncology fellows' clinical experiences during fellowship, perceptions of the intellectual stimulation of their chosen field, and having a supportive mentor have a “significant” influence on the types of patients and conditions they treat after fellowship (hematology, oncology, or both).9 These findings are consistent with other studies that have identified mentorship and networking as critical components to career development within academic medicine.12 Other studies have highlighted the importance of preclinical education, clinical exposure during medical school and residency, and lifestyle factors in positively and sometimes negatively motivating trainees’ decisions to pursue subspecialty training at all, as well as their specialty choices.3,13,14
In light of these findings, we sought to examine the potential roles of medical school, residency, and fellowship experiences, as well as specific mentorship activities, in hematology/oncology fellows’ decisions to pursue hematology-only careers (ie, to practice benign and/or malignant hematology without practicing solid tumor oncology). To study these factors, we conducted a survey, funded by the American Society of Hematology (ASH), which was sent to all fellows in US adult hematology/oncology training programs. We used bivariate and multivariate analyses to explore associations between fellows' training and mentorship experiences and their plans to enter hematology-only careers.
Methods
Participants and study design
The research team developed the 2018 Hematology & Oncology Fellows Survey, an online survey of current adult hematology/oncology fellows, in collaboration with the ASH Recruitment and Retention Working Group, which provided feedback on the survey questions, and members also helped to identify current hematology/oncology fellows to pilot test the survey. The finalized survey included 58 multiple-choice and open-ended survey questions assessing the following domains: current fellowship status, training experiences in hematology and oncology, mentorship experiences, career perceptions, future plans (including intention to practice hematology, oncology, or both), job market experiences including job offers and compensation (for fellows in their third year and beyond), and demographics. The survey questions included in this analysis are shown in supplemental Material.
We sent survey invitations to all current adult hematology/oncology fellows on ASH’s in-training hematology examination list (n = 1899) via e-mail beginning in May 2018. The list included all fellows in ACGME-accredited hematology/oncology and hematology-only fellowship programs, as well as a small number of fellows in non–ACGME-accredited programs including some in their fourth year or beyond of fellowship training. We used the Dillman method to invite participants to complete the survey.15 We sent a prenotification e-mail to potential participants alerting them of the opportunity to complete the survey, followed by an initial survey invitation 2 weeks later. We sent reminders to nonrespondents every 2 weeks after the initial survey invitation, along with additional reminders to fellowship program directors and coordinators to prompt their fellows to complete the survey before the survey closing date in August 2018. Participants who completed the survey (including those who had earlier participated in pilot testing and feedback on the survey questions) received a $10 gift card. We collected all survey data using Qualtrics survey software (Qualtrics, Provo, UT). All survey-related correspondence and the survey instrument itself were cobranded with ASH and George Washington University (GW) logos, but only GW team members had access to the raw survey data to maintain anonymity for survey participants. The study was reviewed and approved by the GW University Office of Human Research.
Study measures
Dependent variable.
Hematology-only career plans: We derived the dependent variable for regression analyses from a survey item that asked, “At this point in your fellowship, which of the following best describes your intended focus post fellowship?” Response options included solid tumor oncology, malignant hematology, and benign hematology along with combinations of the 3 specialty areas and an “I don’t know” option. After excluding responses from fellows who were unsure of their plans, we created a single dichotomous variable indicating plans to enter a hematology-only career (vs a combined or solid tumor oncology-only career) for analysis.
Independent variables.
Medical school experiences (first- and second-year fellows): We created 2 dichotomous variables indicating first- and second-year fellows' exposure to hematology during medical school in the form of (1) participation in an elective hematology or hematology/oncology clerkship and (2) participation in a hematology/oncology rotation during their core internal medicine or pediatrics clerkship. We assumed that exposure to hematology/oncology during a pediatrics clerkship could be related to interest in adult hematology or oncology because of the possibility that trainees might develop interests in these conditions across the life span.
Residency experiences (first- and second-year fellows): We measured fellows' exposure to hematology during residency by asking them to respond to 2 statements using a 5-point Likert scale (strongly disagree to strongly agree): (1) A hematologist encouraged me to pursue a hematology career and (2) I had a clear vision of the career track for becoming a hematologist. We dichotomized responses for analysis (strongly agree or agree vs strongly disagree, disagree or neutral).
Fellowship training experiences.
We used 3 dichotomous variables to measure fellows’ exposure to hematology during fellowship: (1) whether their program director’s clinical and/or research focus was malignant or benign hematology, (2) whether they saw malignant or benign hematology outpatients during their current year of fellowship, and (3) whether their reported patient care time in malignant and benign hematology during the current fellowship year was greater than the median for all respondents.
To gauge fellows' overall perceptions of positive and negative experiences in malignant or benign hematology during fellowship, we created 2 indices quantifying fellows’ positive and negative experiences with malignant or benign hematology during fellowship. The positive experience index (ranging from 0 to 6) included factors such as a large number of intellectually interesting cases and observing providers with good work life balance in malignant or benign hematology, and the negative experience index (ranging from 0 to 4) included factors such as frequent call responsibilities and observing providers experiencing burnout in malignant or benign hematology.
We measured fellows’ participation in hematology research experiences during fellowship through 2 questions: (1) whether they had participated in a malignant or benign hematology research project and (2) whether they had attended a malignant or benign hematology research conference. We collapsed these items into a single dichotomous variable indicating participation in 1 or both research experiences in malignant or benign hematology.
Mentorship.
We measured hematology/oncology fellows’ mentorship experiences in malignant or benign hematology across 4 domains (10 total items): (1) research: coauthored a paper together and/or participated in a research project together; (2) personal connections: invited me for coffee or lunch and/or rounded on patients with me outside of formal training curriculum; (3) networking: introduced me to influential practitioners, helped me to attend conferences, and/or invited me to give presentations at meetings/conferences; and (4) coaching and career advice: helped me make decisions about my career path, suggested positions to apply for, and/or helped me prep for interviews. We collapsed the 10 original items into 4 dichotomous variables indicating whether fellows had experiences in each domain (research, personal connections, networking, and coaching/career advice) with a malignant or benign hematology mentor.
For all fellowship training and mentorship experiences, we asked separately about experiences in malignant and benign hematology and combined responses to questions about both subfields for analysis. We did not define malignant or benign hematology explicitly but allowed fellows to make the distinction between the subfields according to their own understanding.
Control variables.
We included several control variables in the model to account for fellows’ demographic characteristics and underlying interest in hematology before beginning their education. Control variables included interest in hematology before medical school, year of fellowship, age, sex, race/ethnicity (underrepresented in medicine vs not), and international medical graduate status (trained outside the United States and Canada vs trained in the United States or Canada).
Statistical analysis.
We calculated descriptive statistics (mean and standard deviation for continuous variables, frequency distribution for categorical variables) for all study variables. We also conducted bivariate analyses to compare means of continuous variables (using 2-sample Student t tests) and distribution of categorical variables (using Fisher’s exact tests) between fellows with hematology-only and combined or solid tumor oncology-only career plans.
We used 2 logistic regression models to explore associations between fellows’ educational and mentorship experiences and their plans to enter hematology-only careers, holding other experiences, past interest in hematology, and demographic characteristics constant. Model 1 tested associations between fellows’ medical school, residency, and fellowship training and mentorship experiences and their plans to enter hematology-only careers for first- and second-year fellows, who were asked about their experiences across all time periods. (Fellows in their third year and beyond were excluded from this model because they were only asked about their fellowship experiences to minimize recall bias.) Model 2 tested associations between fellows’ fellowship training and mentorship experiences and their plans to enter hematology-only careers for fellows in all years. The null hypothesis for each association tested in the logistic regression analyses was that there was no association between each experience and fellows’ plans to enter a hematology-only career, holding other variables in the model constant (adjusted odds ratio = 1). We used P < .05 as the cutoff for statistical significance. We conducted all statistical analyses in Stata 15 (Stata Corp LLC, College Station, TX).
Results
A total of 850 hematology/oncology fellows responded to the survey (44.7% response rate). Among these, 626 (33.0% of invited participants) had complete data for the variables examined in this study: 207 (33.1%) who planned to enter hematology-only careers, 206 (32.9%) who planned to enter careers including both hematology and solid tumor oncology, and 213 (34.0%) who planned to enter solid tumor oncology–only careers. To check the representativeness of the analysis sample, we compared it with ACGME data on the demographics of all hematology/oncology fellows. The percentages of female (42.3% vs 42%) and international medical graduate (41.2% vs 42%) fellows are nearly the same in the analysis sample relative to ACGME data on all hematology/oncology fellows, suggesting that the sample is representative of the demographics of hematology/oncology fellows.4 The analysis sample slightly overrepresents fellows in their third year of fellowship and beyond (38.3% vs 31.2%), possibly because we included fellows in their fourth year and beyond, some of which are not counted in ACGME data.
Figure 1 shows the breakdown of fellows’ career plans including each possible combination of hematology and oncology subfields. Among all possible combinations, fellows who responded to the survey were most likely to indicate plans to enter solid tumor oncology-only careers (34.0%) and least likely to indicate plans to enter benign hematology-only careers (4.6%). Figure 2 shows the distribution of when fellows reported that they first started seriously considering their chosen subfield(s). The most frequently reported decision point was during residency (32.4%), followed by medical school (29.1%) and fellowship (23.3%). An additional 12.9% of fellows reported first seriously considering their chosen subfield(s) before medical school.
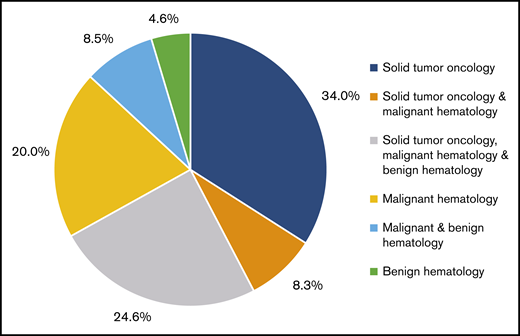
Hematology/oncology fellows’ career plans: at this point in your training, which subfield do you plan to enter? (n = 626).
Hematology/oncology fellows’ career plans: at this point in your training, which subfield do you plan to enter? (n = 626).
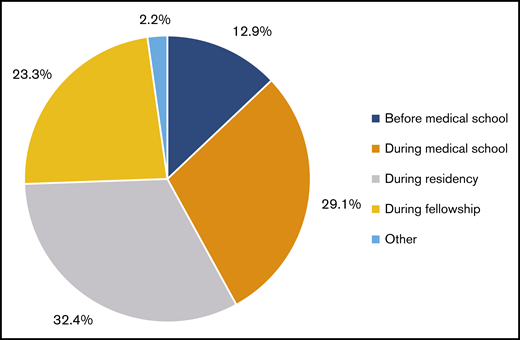
Hematology/oncology fellows’ career plans: when did you first start considering your chosen subfield? (n = 626).
Hematology/oncology fellows’ career plans: when did you first start considering your chosen subfield? (n = 626).
Bivariate analyses
Bivariate analyses suggested that fellows who planned to enter hematology-only careers were significantly more likely to report having training and mentorship experiences in hematology relative to fellows with other career plans throughout their education (Table 1). For example, fellows who planned to enter hematology-only careers were significantly more likely to report completing hematology/oncology rotations in their internal medicine or pediatrics clerkships (45.0% vs 31.4%, P < .05). They were also significantly more likely to report being encouraged to pursue a hematology career (81.8% vs 51.8%, P < .01) and having a clear vision of the hematology career path (78.6% vs 49.4%, P < .01) during their internal medicine residency training.
These trends continued for fellowship training experiences: fellows who planned to enter hematology-only careers were significantly more likely than other fellows to report exposure to hematology outpatients (98.6% vs 88.3%, P < .01), high hematology patient care time (66.2% vs 36.2%, P < .01), and participation in hematology research projects (97.6% vs 60.1%, P < .01). Fellows who planned to enter hematology-only careers also reported significantly higher average numbers of positive (5.12 vs 4.61, P < .01) and negative experiences (2.16 vs 1.91, P < .05) in malignant or benign hematology on the positive and negative fellowship experience indices compared with other fellows.
We found similar patterns with respect to hematology mentorship experiences: fellows who planned to enter hematology-only careers were significantly more likely to report participating in all types of mentorship activities (research, personal, networking, and coaching; P < .01 for each) with hematology mentors relative to fellows with other plans. Fellows planning to enter hematology-only careers also differed from fellows with other plans on several control variables, including having an interest in hematology before medical school (8.2% vs 2.6%, P < .01), first or second year (vs third year) status (P < .05), and underrepresented minority status (13.5% vs 8.1%, P < .05).
Multivariate logistic regression analyses
The 2 multivariate logistic regression analyses we performed to examine training and mentorship experiences and their associations with fellows’ plans to enter hematology-only careers identified several independent associations between specific training experiences and hematology-only career plans, holding other variables constant (Table 2). In model 1, which included data from first- and second-year fellows about their medical school, residency, and fellowship experiences, we found that (1) completing a hematology/oncology rotation in internal medicine or pediatrics clerkship during medical school (odds ratio [OR] = 1.87, P < .05) and (2) having a clear sense of hematology career path during residency (OR = 2.88, P < .01) were significantly and positively associated with plans to enter hematology-only careers. Model 1 also suggested significant and positive associations between (1) high hematology patient care time in current fellowship year (OR = 1.96, P < .01), (2) hematology research experiences (OR = 7.06, P < .01), and (3) conducting research with a hematology mentor (OR = 6.95, P < .01), and plans to enter hematology-only careers.
In model 2, which included data from fellows in all years about their fellowship experiences, we found that plans to enter hematology-only careers were significantly and positively associated with several fellowship experiences: (1) seeing hematology outpatients during current fellowship year (OR = 5.42, P < .05); (2) high hematology patient care time during current fellowship year (OR = 2.07, P < .01); and (3) hematology research project participation (OR = 6.90, P < .01). Among mentorship experiences, the model suggested significant and positive associations with hematology-only career plans for research with a hematology mentor (OR = 5.41, P < .01) and receiving coaching from a hematology mentor (OR = 1.82, P < .05). The other mentorship activities (personal interaction and networking) were not significantly associated with hematology-only career plans in either model.
Discussion
In this large-scale cross-sectional survey study of adult hematology/oncology fellows, we found that experiences in hematology throughout medical school, residency, and fellowship are positively associated with trainees’ interest in pursuing hematology-only careers. Our findings point to several possible avenues for hematology faculty and professional associations to intervene to increase trainees’ exposure to and interest in hematology. For example, there is a significant, positive association between completing a hematology/oncology rotation in an internal medicine or pediatrics clerkship in medical school and hematology-only career plans, even after accounting for prior interest in hematology and subsequent training experiences. This finding aligns with studies of other specialties including primary care and psychiatry, which suggest that many students make their specialty choices in medical school and are often influenced by clerkship experiences, exposure to role models, and opportunities to learn about the patient population a specialty serves.1,16,17
This result is especially interesting because it suggests that exposure to hematology within a core internal medicine or pediatrics clerkship may be more important in influencing trainees’ choices than elective clerkships in hematology and/or oncology (which were not associated with hematology-only career plans). This may mean that increasing hematology faculty participation in core internal medicine or pediatrics clerkships, and by association, the likelihood that medical students will complete a hematology/oncology rotation during their clinical rotations, could help to expand the pipeline of medical students with early exposure to hematology. However, faculty schedules and promotion incentives may not align with emphasis on medical education, especially in a field such as hematology in which most faculty members are also active researchers who may also have extensive demands on their clinical time.18,19 To enable hematologists to participate in undergraduate medical education while balancing competing priorities, academic medical centers may need to find new ways to incentivize hematologists to participate in undergraduate medical education including dedicated time, reduced clinical duties, and salary support.20
The finding that fellows who reported having a clear vision of the hematology career path during their internal medicine residency training were also significantly more likely to indicate plans to enter hematology-only careers underscores the potential importance of residency experiences in shaping trainees’ specialty choices, especially given the prominence of residency as a decision point for trainees who end up pursuing hematology/oncology fellowships. Although it is not exactly known why fellows reported having a clear vision of hematology careers during residency, studies of other specialties have suggested that exposure to role models and research opportunities in a specialty can increase internal medicine residents’ likelihood of pursuing subspecialty training.21-23 Increasing internal medicine residents’ access to hematology role models and research mentors by having more hematologists participate in rounds, lectures, and bedside teaching as part of internal medicine residency training could be another mechanism to increase the pipeline of potential hematologists.
Among fellows who have chosen to pursue hematology/oncology fellowship training, we found that exposure to hematology patients (measured as high hematology patient care time and exposure to hematology outpatients) and research opportunities during fellowship were significantly associated with plans to enter hematology-only careers. This finding likely reflects fellows’ choices to pursue hematology-related training and research opportunities during fellowship to develop their existing interests in hematology, but the strong positive associations of these experiences with hematology-only career plans even when controlling for initial interest in hematology and training and mentorship experiences during medical school and residency suggest that they can reinforce interest in hematology-only careers among fellows who seek them out.
Although fellows with hematology-only career plans reported having significantly more positive and negative clinical experiences queried in the survey, neither positive nor negative experiences related to work schedules, doctor-patient and team relationships, or lifestyle concerns were significantly associated with hematology-only career plans after accounting for other training and mentorship experiences. This finding suggests that perceptions about the quality of clinical experiences or interpersonal care team dynamics may be less important in shaping career decisions for fellows who plan to enter a subspecialty such as hematology than for those who pursue primary care careers, where studies have shown significant associations between doctor-patient and team relationships and lifestyle concerns observed by trainees and their likelihood of entering primary care careers.1,22 Having a fellowship program director whose primary focus was hematology was not predictive of hematology-only career plans either, suggesting that interactions with faculty mentors and research collaborators (regardless of their formal leadership role in the fellowship program) were more important in attracting fellows to hematology than program director subspecialty. This finding suggests that increasing the supply of hematology mentors, even those who are outside of formal leadership positions in fellowship programs or perhaps even at other institutions altogether, could be helpful in increasing the number of fellows who decide to pursue hematology-only careers.
Our findings showing a strong statistical association between hematology mentorship experiences and fellows’ plans to enter hematology-only careers align with other studies that have found that mentorship is 1 of the most important factors in fellows’ specialty choices.9,14 This study builds on previous work by testing associations between specific mentorship experiences and hematology-only career choices; in other words, examining which specific types of interaction with mentors are important in drawing hematology/oncology fellows into hematology-only careers rather than solid tumor oncology careers or career paths that include both hematology and oncology. Bivariate analyses suggest that fellows planning to enter hematology-only careers were significantly more likely to receive mentorship from hematologists in all 4 domains (research, personal connections, networking, and coaching/career advice) compared with their counterparts who planned to enter oncology or combined careers. More important, results of the regression analyses predicting plans to enter hematology-only careers show positive and statistically significant associations between conducting research with and receiving coaching from a hematology mentor, holding other training experiences and control variables constant.
The strong association of research mentorship with hematology/oncology fellows’ interest in pursuing hematology-only careers may be related to the prominence of academic medicine careers in hematology.10,24 Results of a small survey of hematology/oncology fellows trained at the National Cancer Institute–designated cancer centers demonstrated the strong emphasis on academic careers among hematology/oncology fellows, of whom 49% of those surveyed indicated that an academic career was “very important” or “extremely important.”24 Among survey respondents who reported high interest in academic careers, nearly all (90%) reported mentorship to be a key influence in their decision.24 With constrained resources and limited financial incentives, the role of mentorship in stimulating interest and retention in hematology research careers remains crucial for continued progress within the field.
Encouraging fellows and faculty members to participate in formal and informal mentoring relationships can be challenging, especially in resource-constrained environments or institutions with limited hematology faculty.25 However, evidence shows that strong mentoring relationships with clear communication and goals have positive effects on research productivity, personal development, career retention among trainees, and even between fellows and residents.12 Investments in mentorship efforts such as protected time for mentors and/or mentees25 are worthwhile and critical to the success of the specialty in recruiting and developing the next generation of hematologists. Professional associations such as ASH could also play a key role in connecting fellows and faculty members across programs or even between organizations, advocating for increased federal support for research and mentoring grants (eg, Mid-career Investigator Award in Patient-Oriented Research awards) and promoting hematology research opportunities even in hematology/oncology fellowship programs with limited hematology faculty capacity.
This study has several limitations. First, it is a cross-sectional study with self-reported data, including several questions that ask fellows to recall experiences or perceptions from earlier stages in their training. This introduces the possibility that fellows could experience recall bias or project their current interests or plans onto past experiences. We sought to reduce the effect of recall bias by including questions about medical school and residency experiences only for first- and second-year fellows whose memories are more recent, but it is impossible to eliminate it entirely. Also, this study examines associations between fellows’ reported training and mentorship experiences and their career plans only. It cannot provide definitive evidence of a causal relationship between training and mentorship experiences and plans to enter hematology-only careers—or fully account for the possibility that certain training experiences are associated with career plans because fellows choose them already knowing that they plan to enter hematology-only careers. Nonrespondent bias also be could be a factor, but our response rate is consistent with other fellow and physician surveys and our sample appears to be representative of all hematology/oncology fellows according to ACGME data.4,26,27 Additionally, because of the cross-sectional design, we could only examine fellows’ current career intentions rather than their actual job market choices, although evidence from responses of third-year fellows to other survey questions about their job market experiences suggests a strong correlation between fellows’ plans and the jobs they actually take (data not shown). Ongoing efforts to collect longitudinal data from hematology/oncology fellows (and recent fellowship graduates), which are currently under way as part of the broader ASH-GW research project, could help to shed light on the associations between fellows’ training experiences, career choices and job market experiences.
Finally, the wide range of opportunities and career choices for hematology/oncology fellows led us to make a few key assumptions in analyzing the survey data. Because of small numbers of fellows pursuing malignant hematology-only and benign hematology-only careers, we examined malignant and benign hematology experiences and plans together, which may conflate or mask differences between the 2 subfields. Also, our examination of hematology-only career plans as the dependent variable in regression analyses did not consider fellows who could also contribute to the future supply of hematology services through plans to practice hematology in combination with solid tumor oncology. When we examined associations between training and mentorship experiences and plans to practice any hematology (including combined hematology/oncology), we found that many of the associated training and mentorship experiences were consistent for hematology-only and “any hematology” careers, including exposure to hematology patients, hematology research experiences and career coaching from hematology mentors (supplemental Table). These findings suggest that supporting efforts to increase exposure to hematology for students and trainees could help to increase the supply of hematology services through a variety of career pathways for hematology/oncology fellows.
In conclusion, because the hematology workforce seeks to maintain a healthy pipeline of future hematologists in a complex health care and fellowship training environment, this study of factors that are associated with trainees’ career plans can help the field to identify opportunities to attract the next generation of hematologists. Our analyses of Hematology/Oncology Fellows Survey data suggest that increasing clinical exposure to hematology beginning in medical school and connecting trainees with hematology research opportunities and mentors throughout training could have a positive influence on trainees’ likelihood of pursuing hematology-only careers. Given the many competing demands on faculty members’ time, it will be important to continue identifying strategies to increase hematology faculty involvement in medical education and mentorship, as well as connecting trainees with hematology research opportunities and mentors.
Acknowledgments
The authors gratefully acknowledge the help of Emily Bass with survey design and administration and Aleeza-Maria Vitale with manuscript preparation.
Funding for this project was provided by a grant from the American Society of Hematology (ASH). The content of this article is the responsibility solely of the authors and does not necessarily represent official ASH policy.
Authorship
Contribution: L.E.M. designed the survey instrument, collected data, analyzed and interpreted data, conducted statistical analysis, and wrote the manuscript; C.E.E. designed the survey instrument, collected data, analyzed and interpreted data, and provided critical feedback on manuscript; N.T.C., L.M.D.C., G.A.D., A.L.M., R.P.N., M.N., C.L.O., A.R., D.S., and M.S. provided critical feedback on the survey instrument design and manuscript; and A.I.L. designed the survey instrument, analyzed and interpreted data, and provided critical feedback on the manuscript.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Leah E. Masselink, Department of Health Policy and Management, Milken Institute School of Public Health, The George Washington University, 950 New Hampshire Ave NW, Suite 600, Washington, DC 20052; e-mail: lmasselink@gwu.edu.



