

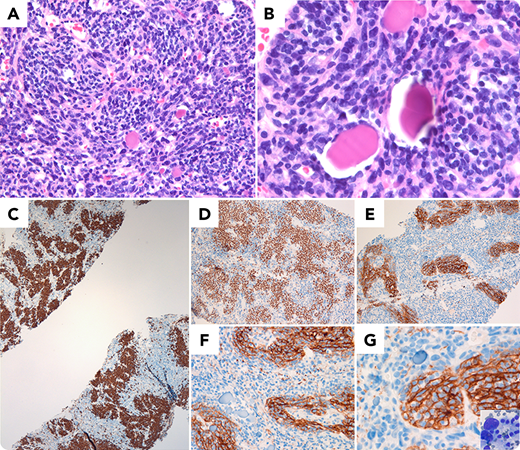
A 52-year-old female presented with an isolated anterior 10-cm mediastinal mass with a normal complete blood count. A core biopsy of the mass revealed a vaguely compartmentalized mononuclear infiltrate (panel A, hematoxylin and eosin) with lymphoid cytomorphology demonstrating occasional streaming. The constituent lymphoid cells were small- to medium-sized (panel B, hematoxylin and eosin) with scattered hyaline globules. Initial workup to exclude lymphoma and thymoma revealed numerous serpiginous clusters of B cells (panel C and D, CD20 immunohistochemistry) with negative CD5, CD10, BCL6, and keratin without evidence of B-cell clonality by polymerase chain reaction. Further workup revealed numerous cells within the nodules positive for follicular dendritic cell (FDC) markers CD21 (panel E, PAX5; panel F, CD21) and CD35 (panel G) with scattered large, atypical cells on Wright-Giemsa stain (panel G, inset), supporting designation as follicular dendritic cell tumor. The diagnosis was confirmed in a subsequent excision of the mass.
The case illustrates an unusual morphologic finding with a reactive, folliculocentric B-cell–rich pattern imparting a serpiginous morphology that can be observed in other neoplasms. These intimately admixed B cells express IgD (and BCL2, not shown) consistent with mantle zone B cells and are not neoplastic. On the other hand, nodal FDC proliferations can also occur in the context of hyaline vascular Castleman disease, but these lesions are not typically folliculocentric. Awareness of these patterns is essential to avoid misdiagnosis as marginal zone lymphoma or follicular lymphoma.
A 52-year-old female presented with an isolated anterior 10-cm mediastinal mass with a normal complete blood count. A core biopsy of the mass revealed a vaguely compartmentalized mononuclear infiltrate (panel A, hematoxylin and eosin) with lymphoid cytomorphology demonstrating occasional streaming. The constituent lymphoid cells were small- to medium-sized (panel B, hematoxylin and eosin) with scattered hyaline globules. Initial workup to exclude lymphoma and thymoma revealed numerous serpiginous clusters of B cells (panel C and D, CD20 immunohistochemistry) with negative CD5, CD10, BCL6, and keratin without evidence of B-cell clonality by polymerase chain reaction. Further workup revealed numerous cells within the nodules positive for follicular dendritic cell (FDC) markers CD21 (panel E, PAX5; panel F, CD21) and CD35 (panel G) with scattered large, atypical cells on Wright-Giemsa stain (panel G, inset), supporting designation as follicular dendritic cell tumor. The diagnosis was confirmed in a subsequent excision of the mass.
The case illustrates an unusual morphologic finding with a reactive, folliculocentric B-cell–rich pattern imparting a serpiginous morphology that can be observed in other neoplasms. These intimately admixed B cells express IgD (and BCL2, not shown) consistent with mantle zone B cells and are not neoplastic. On the other hand, nodal FDC proliferations can also occur in the context of hyaline vascular Castleman disease, but these lesions are not typically folliculocentric. Awareness of these patterns is essential to avoid misdiagnosis as marginal zone lymphoma or follicular lymphoma.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal