

Key Points
Race affects overall relapse risk and response to rituximab in iTTP.
Black patients may require closer monitoring, earlier retreatment, and alternative immunosuppression after rituximab.

Abstract
Immune-mediated thrombotic thrombocytopenic purpura (iTTP) is characterized by recurring episodes of thrombotic microangiopathy, causing ischemic organ impairment. Black patients are overrepresented in iTTP cohorts in the United States, but racial disparities in iTTP outcome and response to therapy have not been studied. Using the United States Thrombotic Microangiopathies Consortium iTTP Registry, we evaluated the impact of race on mortality and relapse-free survival (RFS) in confirmed iTTP in the United States from 1995 to 2020. We separately examined the impact of rituximab therapy and presentation with newly diagnosed (de novo) or relapsed iTTP on RFS by race. A total of 645 participants with 1308 iTTP episodes were available for analysis. Acute iTTP mortality did not differ by race. When all episodes of iTTP were included, Black race was associated with shorter RFS (hazard ratio [HR], 1.60; 95% CI, 1.16-2.21); the addition of rituximab to corticosteroids improved RFS in White (HR, 0.37; 95% CI, 0.18-0.73) but not Black patients (HR, 0.96; 95% CI, 0.71-1.31). In de novo iTTP, rituximab delayed relapse, but Black patients had shorter RFS than White patients, regardless of treatment. In relapsed iTTP, rituximab significantly improved RFS in White but not Black patients. Race affects overall relapse risk and response to rituximab in iTTP. Black patients may require closer monitoring, earlier retreatment, and alternative immunosuppression after rituximab treatment. How race, racism, and social determinants of health contribute to the disparity in relapse risk in iTTP deserves further study.
Introduction
Immune-mediated thrombotic thrombocytopenic purpura (iTTP) is a rare hematologic disorder characterized by life-threatening episodes of microangiopathic hemolytic anemia, thrombocytopenia, and ischemic end-organ impairment. iTTP is caused by an autoantibody-mediated deficiency of the von Willebrand Factor (VWF)–cleaving protease ADAMTS13, resulting in ultralarge VWF multimers, VWF/platelet thrombus development, and microvascular organ damage.1,2 Mortality resulting from acute iTTP has been drastically reduced, from >90% to <10%, with the introduction of therapeutic plasma exchange (TPE), and the addition of caplacizumab is expected to further improve outcome in acute iTTP.3,4 Despite these advances, iTTP remains a chronic relapsing disorder, and each relapse carries significant risk of morbidity and death.5 The use of immunosuppressants likely reduces the risk of relapse; corticosteroids and rituximab are recommended by recent international guidelines.6 However, no large randomized trials exist to confirm the benefit of adding rituximab to treatment for iTTP; rather, only 2 small European single-arm trials have been completed.7,8
In the United States, Black patients are highly overrepresented in iTTP cohorts.9 However, racial disparities in long-term iTTP outcome have not been well studied. A large proportion of observational data and trials informing treatment practices, including the use of rituximab, in iTTP come from European cohorts.7,8 We used the United States Thrombotic Microangiopathies (USTMA) Consortium iTTP Registry, which includes data from 15 high-volume referral centers in the United States and is the largest registry of its kind, to examine racial differences in survival and relapse in iTTP.
Methods
Participant cohort and study outcomes
The study cohort included participants with iTTP treated at the 15 participating USTMA sites from 1990 to 2020. iTTP diagnosis was based on the presence of thrombocytopenia (platelet count <100 × 109/L), microangiopathic hemolytic anemia (hemoglobin below the lower limit of normal, with schistocytes on the peripheral blood smear), and either ADAMTS13 activity <10% or ADAMTS13 activity <20% with an inhibitor or antibody. Participants whose first iTTP episode occurred before 2006, when the ADAMTS13 assay became available, were included only if they had a subsequent relapse with documented ADAMTS13 deficiency. When this criterion was applied, no patients diagnosed before 1995 remained in the cohort, and the cohort for analysis included only episodes occurring between 1995 and 2020. For these participants, data on all available episodes (including episodes before relapse with ADAMTS13 confirmation) of iTTP were recorded. Participants were followed from iTTP diagnosis (or first clinical contact after iTTP diagnosis) until date of death or last contact. Institutional review boards at all participating institutions approved the study. Treatment of participants included daily TPE until a normal platelet count was sustained for at least 2 consecutive days plus immunosuppression. Treatment groups were defined as corticosteroids alone (no specified dose or schedule) or corticosteroids plus 4 doses of rituximab at 375 mg/m2. No participants were treated with caplacizumab.
The primary outcomes of interest were acute iTTP–associated death and relapse-free survival (RFS). Acute iTTP–associated death was recorded if death occurred during hospitalization for iTTP and iTTP was judged as a contributor to or cause of death by the investigator. Non–iTTP-associated death was not recorded. Relapse was defined as recurrence of iTTP after at least 30 days of remission (return to a normal platelet count and lactate dehydrogenase [LDH] level after stopping TPE), and each relapse was treated as an independent event; recurrence within 30 days was considered an exacerbation or continuation of the prior episode.10
Statistical analysis
Data were summarized as counts (and percentages) and means (standard deviations) for categorical and continuous variables, respectively. We used logistic regression to evaluate predictors of mortality resulting from acute iTTP episodes, adding race as a variable to factors previously identified as predictive of mortality.11-13 Predictors of RFS were examined using Cox proportional hazards models for recurrent events.14 Covariates in both models were selected based on biologic plausibility.
To evaluate potential contributors to risk of relapse, including age, sex, occurrence of exacerbation, LDH >10× the upper limit of normal (ULN), first episode (we use the term de novo throughout) vs relapse episode, race, and treatment with rituximab or corticosteroids alone, we used the Prentice-Williams-Peterson gap time approach for modeling time to recurrent events by fitting mixed-effects Cox proportional hazards models, stratified by episode number, with fixed-effects terms for the potential risk factors and random-effects terms for participant and site.
A test for differential treatment effect by race was obtained by including a treatment-by-race interaction term. In analyses of the de novo cohort, participants were followed only until their first relapse, if any, so we fit Cox models without stratifying by episode or including a random effect for participant; any additional episodes were included in the relapsed cohort analysis. Predictors for both models were selected based on biologic plausibility; the LDH criterion was based on a previous report that this conferred a high risk of mortality with acute iTTP episodes.11
The probability of receiving rituximab treatment (propensity score) was estimated for each participant using logistic regression, with symptom severity, laboratory severity (LDH >10× ULN), presence of exacerbation, number of TPEs, and natural cubic spline for calendar year as predictors of treatment assignment. Inverse probability of treatment weights was calculated from the propensity scores.
Based on the findings from the Cox model that race was the strongest risk factor for relapse and that there was a significant treatment-by-race interaction, survival estimates by treatment for each race were examined. Consistent with previous reports, our initial model also suggested that presenting in relapse was a risk factor for relapse,15 so additional analyses separated de novo and relapsed iTTP episodes. Race and treatment emerged as risk factors for relapse for both de novo and relapsed iTTP cohorts; we therefore developed separate models for the de novo and relapsed cohorts to compare RFS by race and treatment (corticosteroids vs corticosteroids plus rituximab). RFS at specific time points (years 1, 3, and 5) was compared using the Klein method, and survival estimates were generated using the Kaplan-Meier estimator.16
We expected that participants with more severe iTTP episodes would be more likely to receive rituximab and that rituximab use would increase over time. Therefore, to account for selection bias, we estimated propensity scores for rituximab treatment using clinical markers of severity and calendar year. We used these propensity scores to adjust the Kaplan-Meier estimates of RFS for treatment selection bias using inverse probability of treatment weighting and compared them with the unweighted estimates.
We examined differences in mortality, treatment, preemptive immunosuppression (defined as therapy administered when ADAMTS13 activity was <10% with a normal platelet count),17 and ADAMTS13 recovery after rituximab to explain the racial disparity. To assess differences in ADAMTS13 recovery, for each episode, we estimated the ADAMTS13 recovery slope using longitudinal linear mixed-effects models to fit a line to each participant’s activity levels between day 1 and day 90 of remission. Then we estimated the relationship between the risk of relapse and ADAMTS13 recovery using joint modeling of longitudinal (ADAMTS13 recovery slope) and time-to-event (relapse) data by race and treatment groups.
Analyses were conducted using R (version 4.0.3), including the packages coxme (version 2.2-16) for mixed-effects Cox models, RISCA (version 0.9) for inverse probability of treatment weighting–adjusted survival curves, and JM (version 1.4-8) for joint models of longitudinal and survival data (R: a language and environment for statistical computing; https://www.r-project.org/; R package coxme [version 2.2-16]: mixed effects Cox models; https://cran.r-project.org/package=coxme; RISCA: causal inference and prediction in cohort-based analyses; https://CRAN.R-project.org/package=RISCA).18
Results
Study cohort
The USTMA Consortium iTTP Registry contains data from 790 unique participants from 15 institutions; 645 met inclusion criteria for this study, with 1049 episodes of iTTP (Figure 1). Table 1 summarizes demographic and clinical characteristics of the cohort by race. Supplemental Figure 6 shows the distribution of race by center.
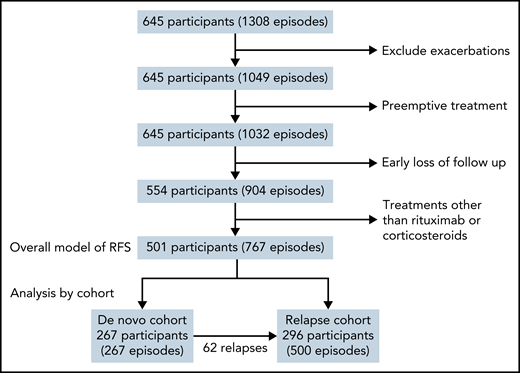
Study cohort. A total of 645 participants in the USTMA Consortium iTTP Registry had a confirmed diagnosis with ADAMTS13 deficiency. An exacerbation was counted as a continuation of the iTTP episode that preceded it. We excluded episodes preceded by preemptive therapy (n = 17), patients lost to follow-up, and patients who received therapy other than corticosteroids or rituximab.
Study cohort. A total of 645 participants in the USTMA Consortium iTTP Registry had a confirmed diagnosis with ADAMTS13 deficiency. An exacerbation was counted as a continuation of the iTTP episode that preceded it. We excluded episodes preceded by preemptive therapy (n = 17), patients lost to follow-up, and patients who received therapy other than corticosteroids or rituximab.
Characteristics of study cohort by race
| All | Black | White | Other/unknown | P | |
|---|---|---|---|---|---|
| No. of patients | 645 | 373 (57.8) | 236 | 36 | |
| No. of episodes | 1049 | 651 (62.1) | 354 | 44 | |
| Sex | .36 | ||||
| Female | 457 (71) | 257 (69) | 175 (74) | 25 (69) | |
| Male | |||||
| Age at time of episode, y | 44 (34, 55) | 44 (35, 56) | 44 (33, 55) | 45 (33, 56) | .73 |
| Episode type | .07 | ||||
| De novo | 358 (34) | 205 (31) | 136 (38) | 17 (39) | |
| Relapsed | 691 (66) | 446 (69) | 218 (62) | 27 (61) | |
| Exacerbation | 201 (19) | 139 (21) | 56 (16) | 6 (14) | .07 |
| LDH >10× ULN | 74 (7) | 53 (8) | 19 (5) | 2 (5) | .24 |
| Treatment | <.0001 | ||||
| Corticosteroids alone | 435 (41) | 284 (44) | 139 (39) | 12 (27) | |
| Rituximab* | 443 (42) | 288 (44) | 132 (37) | 23 (52) | |
| Other | 171 (16) | 79 (12) | 83 (23) | 9 (20) | |
| Follow-up time, y | 2.3 (0.4, 5.5) | 2.7 (0.6, 5.9) | 2.2 (0.1, 5.6) | 1.3 (0.1, 3.5) | .02 |
| All | Black | White | Other/unknown | P | |
|---|---|---|---|---|---|
| No. of patients | 645 | 373 (57.8) | 236 | 36 | |
| No. of episodes | 1049 | 651 (62.1) | 354 | 44 | |
| Sex | .36 | ||||
| Female | 457 (71) | 257 (69) | 175 (74) | 25 (69) | |
| Male | |||||
| Age at time of episode, y | 44 (34, 55) | 44 (35, 56) | 44 (33, 55) | 45 (33, 56) | .73 |
| Episode type | .07 | ||||
| De novo | 358 (34) | 205 (31) | 136 (38) | 17 (39) | |
| Relapsed | 691 (66) | 446 (69) | 218 (62) | 27 (61) | |
| Exacerbation | 201 (19) | 139 (21) | 56 (16) | 6 (14) | .07 |
| LDH >10× ULN | 74 (7) | 53 (8) | 19 (5) | 2 (5) | .24 |
| Treatment | <.0001 | ||||
| Corticosteroids alone | 435 (41) | 284 (44) | 139 (39) | 12 (27) | |
| Rituximab* | 443 (42) | 288 (44) | 132 (37) | 23 (52) | |
| Other | 171 (16) | 79 (12) | 83 (23) | 9 (20) | |
| Follow-up time, y | 2.3 (0.4, 5.5) | 2.7 (0.6, 5.9) | 2.2 (0.1, 5.6) | 1.3 (0.1, 3.5) | .02 |
Data are given as n (%) or median (interquartile range). Sex and follow-up time are summarized per patient; all others are summarized per episode.
Of 443 episodes treated with rituximab, 426 (96.2%) were treated with 375 mg/m2 for 4 weekly doses and 15 (3.4%) with 375 mg/m2 for 4 doses on days 1, 4, 8, and 15; 2 (0.5%) were treated with a combination of the 2 regimens.
Race- and iTTP-associated mortality
Acute iTTP-associated death occurred in 35 (3.3%) of 1049 episodes: 21 (3.2%) of 651 episodes in Black patients, 13 (3.7%) of 354 episodes in White patients, and 1 (2.3%) of 44 episodes in patients of other/unknown race. A logistic regression model for mortality, including race, age, sex, de novo status, exacerbation, and LDH >10× ULN, did not show a significant effect of race (White vs Black: OR, 1.03; 95% CI, 0.49-2.16; P = .94; other/unknown vs Black: OR, 0.69; 95% CI, 0.09-5.25; P = .72). Age (OR per 10 years, 1.53; 95% CI, 1.21-1.93; P < .001), male sex (OR, 2.90; 95% CI, 1.44-5.84; P < .001), and de novo episode (OR, 2.12; 95% CI, 1.00-4.52; P = .051) were most strongly associated with mortality (Figure 2).

Risk factors for mortality in patients presenting with de novo or relapsed iTTP. A multivariate model of mortality from iTTP failed to demonstrate an effect of race on mortality. Minor edits made with Biorender.com.
Risk factors for mortality in patients presenting with de novo or relapsed iTTP. A multivariate model of mortality from iTTP failed to demonstrate an effect of race on mortality. Minor edits made with Biorender.com.
Race and RFS
Relapses of iTTP occurred in 34% (218 of 645) of participants overall, including in 40% (150 of 373) of Black patients, 26% (62 of 236) of White patients, and 17% (6 of 36) of patients of other/unknown race. We excluded participants who were followed for <90 days, received treatment other than either corticosteroids or rituximab, or received preemptive immunosuppressive therapy (Figure 1). In the Cox proportional hazards model evaluating predictors of RFS, 501 unique participants were included. Black race was associated with shorter RFS, even after adjusting for treatment (corticosteroids vs corticosteroids plus rituximab; Figure 3).

Risk factors for iTTP relapse. A multivariate model of relapse identified race as the strongest predictor of relapse, along with a significant effect of previous relapse and a trend toward treatment with rituximab being protective against relapse. Minor edits made with Biorender.com. HR, hazard ratio.
Risk factors for iTTP relapse. A multivariate model of relapse identified race as the strongest predictor of relapse, along with a significant effect of previous relapse and a trend toward treatment with rituximab being protective against relapse. Minor edits made with Biorender.com. HR, hazard ratio.
Based on these initial results, we examined RFS by race and treatment in further detail. Rituximab (vs corticosteroids alone) improved RFS in White patients (with de novo or relapsed iTTP; HR, 0.37; 95% CI, 0.18-0.73; P = .0044; 5-year RFS, 78% vs 48%) but did not seem to improve RFS in Black patients (HR, 0.96; 95% CI, 0.71-1.31; P = .81; 5-year RFS, 36% vs 43%; Figure 4A). The treatment-by-race interaction test in this analysis indicated that the relationship between treatment and RFS differed by race (P < .001). The lack of improvement in RFS in Black patients receiving rituximab was unexpected, so we then analyzed RFS by race separately for de novo or relapsed iTTP cohorts because previous reports suggested presenting in relapse is a major risk factor for subsequent relapse.

Effect of race and rituximab therapy on RFS in patients presenting with de novo or relapsed iTTP. (A) Overall, Black patients had shorter time to relapse compared with White patients, regardless of treatment. (B) A wearing-off effect of rituximab was found in de novo iTTP, with Black patients seeming to lose the protective effect of rituximab faster than White patients. (C) A pronounced interaction between race and treatment was evident in relapsed iTTP episodes, where RFS more than doubled in White patients with the addition of rituximab. There was no difference in RFS in relapsed iTTP in Black patients, whether treated with rituximab or corticosteroids alone. Minor edits made with Biorender.com.
Effect of race and rituximab therapy on RFS in patients presenting with de novo or relapsed iTTP. (A) Overall, Black patients had shorter time to relapse compared with White patients, regardless of treatment. (B) A wearing-off effect of rituximab was found in de novo iTTP, with Black patients seeming to lose the protective effect of rituximab faster than White patients. (C) A pronounced interaction between race and treatment was evident in relapsed iTTP episodes, where RFS more than doubled in White patients with the addition of rituximab. There was no difference in RFS in relapsed iTTP in Black patients, whether treated with rituximab or corticosteroids alone. Minor edits made with Biorender.com.
Effect of race, prior relapse, and treatment on RFS
Survival analyses of de novo and relapsed iTTP cohorts are presented in supplemental Figure 7. The de novo iTTP cohort included 267 patients, and the relapsed iTTP cohort included 296 patients (including 62 patients of the original de novo iTTP cohort who relapsed during follow-up). In the de novo cohort, overall RFS was significantly longer in participants treated with rituximab compared with those treated with corticosteroids alone (HR, 0.57; 95% CI, 0.35-0.92; P = .022). However, when we examined RFS using the Klein method, rituximab improved RFS at 1 year (92% vs 79%; P = .0017) and 3 years (78% vs 63%; P = .022) but not 5 years (59% vs 55%; P = .62), which suggests the effect wears off over time. In the relapsed iTTP cohort, rituximab was not associated with longer overall RFS (HR 0.86 (0.61–1.20), P = .37); however, RFS was higher in the rituximab group at 1 year (82% vs 72%; P = .01) but not at 3 years (53% vs 46%; P = .19) or 5 years (41% vs 40%; P = .81), suggesting that benefit, if any, is shorter lived in relapsed iTTP. On analyzing the cohorts separately by race, an interaction between race and treatment was observed in the relapsed cohort (P = .0035) but not in the de novo cohort (P = .45).
Given the treatment and race interaction, we then analyzed RFS in subcohorts of relapse status and race by treatment: de novo and White, de novo and Black, relapsed and White, and relapsed and Black participants (Figure 4B-C). In White participants with de novo iTTP, rituximab was not associated with improved overall RFS (HR, 0.47; 95% CI, 0.16-1.41; P = .18). When separate time points were analyzed, there was no difference in RFS at 1 year (93% vs 88%; P = .40), 3 years (82% vs 70%; P = .29), or 5 years (82% vs 61%; P = .10). In Black participants with de novo iTTP, rituximab did not improve overall RFS (HR, 0.70; 95% CI, 0.40-1.20; P = .20). RFS was improved at 1 year (91% vs 76%; P = .0064) but not at 3 years (75% vs 60%; P = .080) or 5 years (47% vs 52%; P = .68).
In relapsed iTTP (500 episodes in 296 participants), rituximab significantly improved RFS among White participants (HR, 0.26; 95% CI, 0.09-0.77; P = .015) but not among Black participants (HR, 1.08; 95% CI, 0.74-1.58; P = .69; Figure 4C). In White patients, RFS with rituximab compared with corticosteroids alone was 95% vs 71% at 1 year (P < .0001), 79% vs 44% at 3 years (P = .00012), and 75% vs 40% at 5 years (P = .00033). In Black patients, RFS with rituximab compared with corticosteroids alone was 77% vs 72% at 1 year (P = .29), 44% vs 47% at 3 years (P = .69), and 31% vs 38% at 5 years (P = .28).
Effect of selection bias on RFS
Treatment propensity scores were created for episodes treated by rituximab and corticosteroids or corticosteroids alone. An increasing proportion of episodes were treated with rituximab over time (Figure 5), and participants with more severe episodes were more likely to be treated with rituximab (supplemental Figure 8). However, when we adjusted our models using inverse probability treatment weighting, we observed little change in 5-year RFS curves (supplemental Figure 9).

Treatment selection over time. The use of rituximab for treatment of iTTP increased steadily over time starting with its introduction in the early 2000s.
Treatment selection over time. The use of rituximab for treatment of iTTP increased steadily over time starting with its introduction in the early 2000s.
We next examined differences in access to care and treatment patterns. The proportion of episodes treated with rituximab did not differ between Black and White participants (51% vs 47%; P = .34). There was no significant difference in the proportion of episodes treated with preemptive therapy between races (Black, 1.8%; other/unknown, 2.3%; White, 1.1%; P = .41).
Early ADAMTS13 recovery and relapse
ADAMTS13 activity levels after iTTP remission were available for 128 iTTP episodes, 103 of which were treated with rituximab, 28 in the de novo group and 75 in the relapsed group (Table 2). Overall, faster ADAMTS13 recovery in the first 3 months was protective against relapse (HR, 0.79 for each 0.25 rise in slope [rise ADAMTS13 activity per day]; 95% CI, 0.64-0.98; P = .03). However, when only iTTP episodes treated with rituximab were included, the slope of ADAMTS13 recovery was not associated with relapse overall or within de novo and relapsed groups. We found no differences in rate of ADAMTS13 recovery by race or treatment. We could not evaluate the association of durability of ADAMTS13 response with RFS because of the sparsity of data points (ADAMTS13) at >1 year from the acute episode.
Rate of early ADAMTS13 recovery and relapse
| No. of episodes | Mean ADAMTS13 recovery slope | 95% CI | P | |
|---|---|---|---|---|
| Treatment | .11 | |||
| Rituximab | 103 | 0.9 | 0.82-0.99 | |
| Corticosteroids alone | 13 | 0.96 | 0.73-1.19 | |
| Other | 12 | 0.65 | 0.39-0.90 | |
| Race | .89 | |||
| Black | 79 | 0.88 | 0.79-0.98 | |
| White | 43 | 0.91 | 0.76-1.06 | |
| Other/unknown | 6 | 0.96 | 0.61-1.32 | |
| No. of episodes | HR (per +0.25 increase in ADAMTS13 recovery slope) | 95% CI | P | |
| All | 128 | 0.79 | 0.64-0.98 | .03 |
| Rituximab only | 103 | 0.92 | 0.71-1.18 | .5 |
| De novo, rituximab | 28 | 0.58 | 0.18-1.83 | .35 |
| Relapsed, rituximab | 75 | 0.99 | 0.75-1.31 | .94 |
| No. of episodes | Mean ADAMTS13 recovery slope | 95% CI | P | |
|---|---|---|---|---|
| Treatment | .11 | |||
| Rituximab | 103 | 0.9 | 0.82-0.99 | |
| Corticosteroids alone | 13 | 0.96 | 0.73-1.19 | |
| Other | 12 | 0.65 | 0.39-0.90 | |
| Race | .89 | |||
| Black | 79 | 0.88 | 0.79-0.98 | |
| White | 43 | 0.91 | 0.76-1.06 | |
| Other/unknown | 6 | 0.96 | 0.61-1.32 | |
| No. of episodes | HR (per +0.25 increase in ADAMTS13 recovery slope) | 95% CI | P | |
| All | 128 | 0.79 | 0.64-0.98 | .03 |
| Rituximab only | 103 | 0.92 | 0.71-1.18 | .5 |
| De novo, rituximab | 28 | 0.58 | 0.18-1.83 | .35 |
| Relapsed, rituximab | 75 | 0.99 | 0.75-1.31 | .94 |
Discussion
In the largest multicenter study of iTTP in the United States, we identify for the first time an important racial disparity in iTTP outcomes between Black and White patients. Black race is associated with higher relapse risk, even after adjusting for treatment with rituximab and selection bias. Although treatment with rituximab delays relapse in de novo iTTP, Black patients had shorter RFS than White patients regardless of treatment. Importantly, in relapsed iTTP, rituximab significantly improved RFS in White but not in Black patients. This suggests that in relapsed iTTP, Black patients in particular are more likely to have a much shorter-lived response to rituximab and benefit from closer monitoring and consideration of alternative immunosuppressive therapies.
Rituximab is recommended by the recent International Society on Thrombosis and Haemostasis guidelines on iTTP management and is widely used for the treatment of iTTP.6 A French series of 22 patients with refractory iTTP treated with rituximab reported improved RFS at 1 year compared with historical patients but no difference after 1 year, and a phase 2 single-arm trial with 40 participants from the United Kingdom showed a reduction in 5-year relapse rate to 10% from 57% in historical controls.7,19 A report from the Oklahoma TTP registry in de novo iTTP (n = 16; 14 with refractory iTTP) demonstrated improved RFS over those treated with corticosteroids alone (n = 21).20 Our findings likely differ from these previous reports because our cohort is much larger and had long-term follow-up but also because racial constructs and the effect of race on health may differ between Europe and the United States. Rituximab clearly improves RFS in some patients, and we do not advocate for withholding rituximab based on these results. However, our results indicate that the relapse-preventing effect of rituximab seems to be shorter lived in Black patients, especially those with relapsed iTTP. These patients will require closer monitoring and consideration of repeat courses of rituximab or alternative immunosuppression if rituximab does improve ADAMTS13 activity. This is consistent with another recent US report that rituximab delays but does not prevent relapse in iTTP.15 One hypothesis regarding the attenuated benefit of rituximab in some patients with relapsed iTTP is that B cells may mature to long-lived plasma cells that are not targeted by rituximab but may respond to therapies such as bortezomib and daratumumab.21-24
To test potential contributors to this racial disparity, we evaluated access to care, measured by iTTP-related mortality and use of preventive immunosuppression. We found that iTTP-related mortality and use of preemptive therapy do not explain the higher relapse risk and attenuated response to rituximab in Black patients with iTTP in our cohort. In fact, the proportion of episodes treated with rituximab and preemptive immunosuppression were higher for Black patients. We also evaluated whether the early immunosuppressive effect of rituximab reflected in ADAMTS13 recovery differed by race. However, most individuals recovered ADAMTS13 activity to >25% by 90 days, and there was no difference in early ADAMTS13 recovery by race.
Racial disparities in long-term response to rituximab have not previously been studied in iTTP. We hypothesize that B-cell depletion by rituximab is shorter lived in Black patients but were unable to examine this in our retrospective data set. However, Black patients had significantly faster B-cell repletion after anti-CD20 therapy in a cohort of patients with multiple sclerosis and neuromyelitis optica.25 Other studies suggest more robust B-cell responses in African American patients with autoimmune disorders, including multiple sclerosis and lupus.26,27 Trials of rituximab in systemic lupus erythematosus also support these findings. Trials conducted in Europe, with smaller proportions of Black patients, have demonstrated greater benefit compared with results in the United States, suggesting shared immune mechanisms of refractoriness among patients with lupus and iTTP.28,29 Understanding biologic differences in response to targeted immune therapies is critical to improving outcome in iTTP.
Other genetic and environmental factors may contribute to the higher iTTP relapse rate in Black patients (eg, a lower frequency of the HLA-DRB1*04 allele that is protective against iTTP30). It is also plausible that exposure to ADAMTS13 epitopes from predominantly White blood donors during TPE leads to a differential alloimmune boost of ADAMTS13 antibodies and epitope spreading that mirror the higher rate of alloantibody formation in Black patients after red blood cell transfusion.31,32 Finally, although ADAMTS13 activity in remission is a logical biomarker for relapse, reports on its prediction strength are conflicting.33-35 Other non–ADAMTS13-dependent mechanisms likely play a role in relapse. These may include blood type (a surrogate for VWF level)15 or differing thresholds for complement activation by ultralarge VWF.36 Race and race-associated biologic, social, and health care disparities may be key clues to unveiling these risk factors.
Strengths of this study include the large number of participants representative of the iTTP population in the United States; this is the largest reported US cohort and among the largest in the world. Limitations include loss to follow-up and absence of long-term ADAMTS13 data and biologic samples that limit our mechanistic conclusions and the fact that rituximab therapy was not randomized. Because patients diagnosed between 1990 and 2006 were included only if they survived to have a relapse after 2006, and those with fatal episodes occurring before 2006 were excluded, the mortality rate in this cohort may have been underestimated. Selection bias is a concern common to all observational studies; however, our conclusions remained valid after we adjusted for selection bias using propensity scores for treatment selection. Current efforts of the USTMA Consortium focus on prospective studies of long-term outcome in iTTP.
In conclusion, we report a novel and important effect of race on relapse risk and response to rituximab in iTTP. Black patients with iTTP, particularly those with relapsed disease, may have suboptimal responses to rituximab and may require closer monitoring and other immunosuppressive therapies. There is a critical need to investigate the mechanisms underlying the observed differences in natural history and response to therapy between Black and White patients, including how genetic and environmental factors affect disease biology. Understanding these contributors to relapse will aid in developing personalized strategies to improve long-term outcomes in all patients with iTTP.
Acknowledgments
This study was supported by grants K99HL150594 (S.C.) and UL1TR001111 and UL1TR002494, the National Institutes of Health Clinical and Translational Science Awards to the University of North Carolina at Chapel Hill and the University of Minnesota, for data maintenance and security of the REDCap databases used to house the data for this study. No industry support was provided. The visual abstract was created with Biorender.com.
Authorship
Contribution: S.C. contributed to the design of the study and data acquisition and interpretation, drafted the manuscript, and approved the final version of the manuscript. M.D.E. and M.A.M. designed the study, accessed and verified data, analyzed and interpreted the data, drafted the manuscript, and approved the final version of the manuscript. A.G.A., A.M.F., R.W., A.M., Y.A.P., G.d.R., B.G., R.S.K., D.K.L, F.A., T.C., L.B.K., M.S., R.S.G., K.R.M., A.L., M.Y.L., R.G., X.L.Z., J.S.R., C.M., S.R.C., A.J., H.V.U., and E.D. contributed to data acquisition and approved the final version of the manuscript. J.E.S. contributed to data acquisition.
Conflict-of-interest disclosure: S.C. reports advisory board participation for Alexion, Sanofi Genzyme, Sobi, and UCB Pharma. R.W. reports advisory board participation for Sanofi Genzyme. A.M. reports payment for lectures and travel by Sanofi Genzyme. G.d.R. reports advisory board participation for Sanofi Genzyme. J.S.R. reports advisory board participation for Sanofi Genzyme. K.R.M. reports consulting for Sanofi Genzyme. M.S. reports advisory board participation for Alexion. R.G. reports consulting for Sanofi Genzyme and Alexion. X.L.Z. reports consulting for Alexion, Takeda, and Sanofi Genzyme. C.M. reports advisory board participation for Takeda and Sanofi Genzyme. M.A.M. reports payment for lectures and travel by Sanofi Genzyme. The remaining authors declare no competing financial interests.
J. Evan Sadler died on 13 December 2018.
A complete list of the members and participating sites of the United States Thrombotic Microangiopathies Consortium appears in the supplemental appendix.
Correspondence: Marshall A. Mazepa, University of Minnesota Medical School, 516 Delaware St SE, Mayo Code 480, Minneapolis, MN 55455; e-mail: mmazepa@umn.edu.
Presented in part in abstract form at the 61st Annual Meeting of the American Society of Hematology, Orlando, FL, 8 December 2019.
The online version of this article contains a data supplement.
There is a Blood Commentary on this article in this issue.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal