

A 63-year-old woman with a long-standing history of pancreatic pseudocyst underwent resection due to worsening symptoms. Microscopic examination of the pseudocyst incidentally revealed a few aggregates of large cells within the fibrin surrounding the cyst wall (panel A; 10× objective, total magnification ×100; panel B; 40× objective, total magnification ×400; Hematoxylin and Eosin stain). By immunohistochemistry, these cells were positive for CD45, CD20 (panel C), CD4 (panel E), PAX5, MUM-1, and EBER (panel F), whereas they were negative for CD3 (panel D), CD10, BCL-6, CD30, HHV8, AE1/AE3, S100, synaptophysin, and MART1 (panels C-F; 20× objective, total magnification ×200). The CD4 positivity prompted additional workup to exclude T-cell lymphoma, blastic plasmacytoid dendritic cell neoplasm (BPDCN), myeloid sarcoma with monocytic differentiation, and an HHV8+plasmablastic neoplasm with aberrant T-antigen expression. The cells were negative for all other T-cell markers (CD3, CD2, CD5, CD7, CD25), BPDCN markers (CD56, CD123, TCL-1), myeloid markers (CD117, CD34, MPO, CD68, CD43), and HHV8. Hence, a diagnosis of fibrin-associated diffuse large B-cell lymphoma (FA-DLBCL) with aberrant CD4 expression was made.
FA-DLBCL is an unusual Epstein-Barr virus–positive DLBCL found incidentally within fibrin-rich restricted anatomic spaces in immunocompetent individuals. Previously considered a form of DLBCL-chronic inflammation (CI), its distinct features now merit separate classification in the World Health Organization 5th edition. Our case suggests that aberrant T-cell antigen expression, known to occur in DLBCL-CI, may rarely be seen in FA-DLBCL.
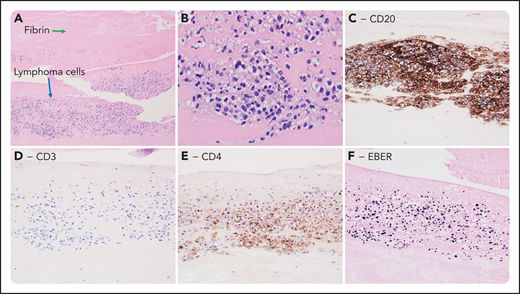
A 63-year-old woman with a long-standing history of pancreatic pseudocyst underwent resection due to worsening symptoms. Microscopic examination of the pseudocyst incidentally revealed a few aggregates of large cells within the fibrin surrounding the cyst wall (panel A; 10× objective, total magnification ×100; panel B; 40× objective, total magnification ×400; Hematoxylin and Eosin stain). By immunohistochemistry, these cells were positive for CD45, CD20 (panel C), CD4 (panel E), PAX5, MUM-1, and EBER (panel F), whereas they were negative for CD3 (panel D), CD10, BCL-6, CD30, HHV8, AE1/AE3, S100, synaptophysin, and MART1 (panels C-F; 20× objective, total magnification ×200). The CD4 positivity prompted additional workup to exclude T-cell lymphoma, blastic plasmacytoid dendritic cell neoplasm (BPDCN), myeloid sarcoma with monocytic differentiation, and an HHV8+plasmablastic neoplasm with aberrant T-antigen expression. The cells were negative for all other T-cell markers (CD3, CD2, CD5, CD7, CD25), BPDCN markers (CD56, CD123, TCL-1), myeloid markers (CD117, CD34, MPO, CD68, CD43), and HHV8. Hence, a diagnosis of fibrin-associated diffuse large B-cell lymphoma (FA-DLBCL) with aberrant CD4 expression was made.
FA-DLBCL is an unusual Epstein-Barr virus–positive DLBCL found incidentally within fibrin-rich restricted anatomic spaces in immunocompetent individuals. Previously considered a form of DLBCL-chronic inflammation (CI), its distinct features now merit separate classification in the World Health Organization 5th edition. Our case suggests that aberrant T-cell antigen expression, known to occur in DLBCL-CI, may rarely be seen in FA-DLBCL.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal