

TO THE EDITOR:
CD19 -specific chimeric antigen receptor (CAR19) T cells induce remission of B cell malignancy,1-6 but manufacture of individualized autologous products with viral vectors is expensive,7 delays treatment, risks contamination with malignant B cells,8 and is not feasible in patients with insufficient healthy T cells.9 Generation of CAR19 T cells using an allogeneic donor is a promising alternative strategy, but limited data exist regarding safety and efficacy.1-3,10,11
We report first-in-human administration of CAR19 T cells manufactured using the piggyBac transposon system, an inexpensive, high-capacity, nonviral alternative for CAR T-cell generation.12-14 Patients with relapsed or refractory CD19+ malignancy following HLA-matched sibling donor hematopoietic stem cell transplant (HSCT) were assessed for enrollment in a phase 1 clinical trial of escalating doses of HSCT donor-derived allogeneic piggyBac CAR19 T cells (registered at www.anzctr.org.au as ACTRN12617001579381) (Figure 1A and supplemental Methods, available on the Blood Web site). All 10 treated patients (Table 1) were included in this analysis irrespective of trial inclusion (supplemental Figure 1).
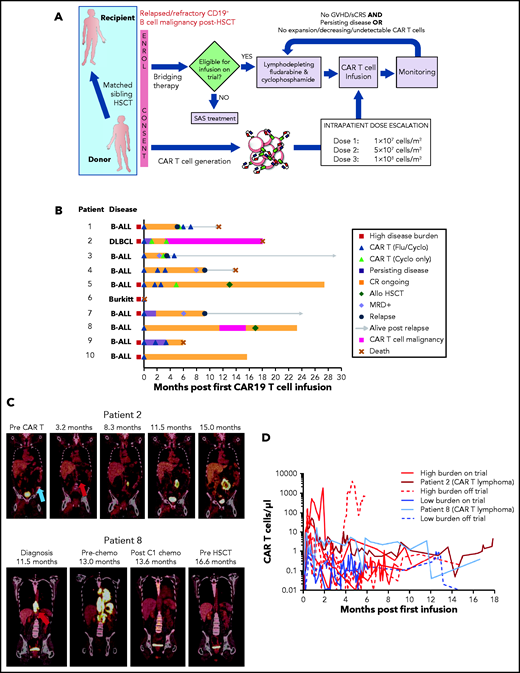
Patient outcomes and piggyBac CAR19 T-cell expansion and persistence after infusion of escalating doses. (A) Clinical trial schema. Patients with relapsed or refractory B-cell malignancies post–allogeneic HSCT (Allo HSCT) received up to 3 escalating doses of HLA-matched sibling donor-derived piggyBac CAR19 T cells at least 1 month apart. Trial eligibility was assessed at enrollment and immediately before infusion. Those ineligible for infusion could elect to receive CAR19 T cells under the Therapeutic Goods of Australia Special Access Scheme (SAS) off-trial. (B) Swimmer plot showing disease response to escalating doses of donor-derived piggyBac CAR19 T cells in each patient. (C) Serial PET-CT scan images showing development of CAR19 T-cell lymphoma in 2 patients in CR of B cell malignancy. Patient 2 died of complications of CAR19 T-cell lymphoma and its treatment; patient 8 achieved CR of CAR19 T-cell lymphoma with 4 cycles of augmented CHOP chemotherapy, and remains in CR post–second allogeneic HSCT. Blue arrow, site of original disease for patient 2; red arrows, sites of CAR T-cell lymphoma for each patient. (D) Donor-derived piggyBac CAR19 T-cell expansion and persistence in the peripheral blood of each patient was assessed by flow cytometry. Data for the 2 patients who developed a CAR T-cell lymphoma are highlighted. chemo, chemotherapy; Cyclo, cyclophosphamide; DLBCL, diffuse large B-cell lymphoma; Flu, fludarabine; sCRS, severe CRS.
Patient outcomes and piggyBac CAR19 T-cell expansion and persistence after infusion of escalating doses. (A) Clinical trial schema. Patients with relapsed or refractory B-cell malignancies post–allogeneic HSCT (Allo HSCT) received up to 3 escalating doses of HLA-matched sibling donor-derived piggyBac CAR19 T cells at least 1 month apart. Trial eligibility was assessed at enrollment and immediately before infusion. Those ineligible for infusion could elect to receive CAR19 T cells under the Therapeutic Goods of Australia Special Access Scheme (SAS) off-trial. (B) Swimmer plot showing disease response to escalating doses of donor-derived piggyBac CAR19 T cells in each patient. (C) Serial PET-CT scan images showing development of CAR19 T-cell lymphoma in 2 patients in CR of B cell malignancy. Patient 2 died of complications of CAR19 T-cell lymphoma and its treatment; patient 8 achieved CR of CAR19 T-cell lymphoma with 4 cycles of augmented CHOP chemotherapy, and remains in CR post–second allogeneic HSCT. Blue arrow, site of original disease for patient 2; red arrows, sites of CAR T-cell lymphoma for each patient. (D) Donor-derived piggyBac CAR19 T-cell expansion and persistence in the peripheral blood of each patient was assessed by flow cytometry. Data for the 2 patients who developed a CAR T-cell lymphoma are highlighted. chemo, chemotherapy; Cyclo, cyclophosphamide; DLBCL, diffuse large B-cell lymphoma; Flu, fludarabine; sCRS, severe CRS.
Clinical characteristics of patients administered escalating doses of piggyBac CAR19 T cells
| No. | Sex, age (y) | Disease | Primary refractory? | Prior auto | Matched related allo conditioning | DLI? | Prior blin? | Total prior lines of therapy | Status at first dose CAR T | Treated on-trial? (reason off) | CAR19 T-cell doses administered (preceding lymphodepletion) | Best response* (dose no. achieved) | Duration of response, mo | CRS† | ICANS‡ | Other adverse events |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F, 25 | B-ALL | No | No | MAC | No | Yes | 5 | Extra-medullary | Yes | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Cy) 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Flu/Cy) | MRD− CR (1) | 5.1 | Gr 1 | No | Cytopenias requiring support Urosepsis Death from PD |
| 2 | M, 66 | DLBCL | Yes | BEAM | RIC | 3 | No | 8 | Stage IV | Yes | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Cy) 1 × 108 TNC/m2 (Cy) | CR (2) | 18.0§ | No | No | Worsening cGVHD Pneumonia CVAD sepsis GI sepsis Death from CAR T cell malignancy‖ |
| 3 | M, 61 | B-ALL | No | No | RIC | No | No | 4 | MRD+ | Yes | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Cy) 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Flu/Cy) | MRD− CR (1) | 3.5 | No | No | Cytopenias requiring support |
| 4 | M, 42 | B-ALL | No | No | MAC | No | Yes | 5 | MRD− | No (prior seizures) | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Flu/Cy) | MRD− CR (1) | 9.2 | No | No | Cytopenias requiring support CVAD sepsis Death from PD |
| 5 | M, 18 | B-ALL | No MRD+ | No | MAC | 3 | Yes | 5 | Blasts 70% | No (IFI) | 1 × 107 TNC/m2 (Flu/Cy) 1 × 107 TNC/m2 (Flu/Cy)¶ 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Cy)# | MRD− CR (1) | 27.4§ | Gr 2 | No | Cytopenias requiring support |
| 6 | M, 18 | Burkitt | Yes | BEAM | RIC | No | No | 6 | Stage IV | No (ECOG 3) | 1 × 107 TNC/m2 (Flu/Cy) | N/A | N/A | N/A | N/A | Death from pulmonary embolus |
| 7 | M, 47 | B-ALL | No, MRD+ | No | MAC | No | Yes | 4 | BM: MRD− Occult extra-medullary | Yes | 1 × 107 TNC/m2 (Flu/Cy) | MRD− CR (1) | 9.2 | Gr 2 | No | Cytopenias requiring support |
| 8 | M, 30 | B-ALL | No | No | MAC | No | Yes | 5 | MRD+ | Yes | 1 × 107 TNC/m2 (Flu/Cy) | MRD− CR (1) | 23.2§ | No | No | CAR T malignancy Cytopenias requiring support |
| 9 | M, 20 | B-ALL | No, MRD+ | No | (1) MAC (2) MAC | 2 | No | 8 | Cerebellar mass | No (release criteria**) | 1 × 107 cells/m2 (Flu/Cy) 5 × 107 cells/m2 (Flu/Cy) 1 × 108 cells/m2 (Flu/Cy) | CR (3) | 6.0§ | Gr 2 | No | Cytopenias requiring support CVAD sepsis Death from multiviral SIRS‖ |
| 10 | F, 62 | B-ALL | No | No | RIC | No | No | 4 | Extra-medullary | Yes | 1 × 107 cells/m2 (Flu/Cy) | CR (1) | 15.6§ | No | No | Cytopenias requiring support |
| No. | Sex, age (y) | Disease | Primary refractory? | Prior auto | Matched related allo conditioning | DLI? | Prior blin? | Total prior lines of therapy | Status at first dose CAR T | Treated on-trial? (reason off) | CAR19 T-cell doses administered (preceding lymphodepletion) | Best response* (dose no. achieved) | Duration of response, mo | CRS† | ICANS‡ | Other adverse events |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F, 25 | B-ALL | No | No | MAC | No | Yes | 5 | Extra-medullary | Yes | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Cy) 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Flu/Cy) | MRD− CR (1) | 5.1 | Gr 1 | No | Cytopenias requiring support Urosepsis Death from PD |
| 2 | M, 66 | DLBCL | Yes | BEAM | RIC | 3 | No | 8 | Stage IV | Yes | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Cy) 1 × 108 TNC/m2 (Cy) | CR (2) | 18.0§ | No | No | Worsening cGVHD Pneumonia CVAD sepsis GI sepsis Death from CAR T cell malignancy‖ |
| 3 | M, 61 | B-ALL | No | No | RIC | No | No | 4 | MRD+ | Yes | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Cy) 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Flu/Cy) | MRD− CR (1) | 3.5 | No | No | Cytopenias requiring support |
| 4 | M, 42 | B-ALL | No | No | MAC | No | Yes | 5 | MRD− | No (prior seizures) | 1 × 107 TNC/m2 (Flu/Cy) 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Flu/Cy) | MRD− CR (1) | 9.2 | No | No | Cytopenias requiring support CVAD sepsis Death from PD |
| 5 | M, 18 | B-ALL | No MRD+ | No | MAC | 3 | Yes | 5 | Blasts 70% | No (IFI) | 1 × 107 TNC/m2 (Flu/Cy) 1 × 107 TNC/m2 (Flu/Cy)¶ 5 × 107 TNC/m2 (Flu/Cy) 1 × 108 TNC/m2 (Cy)# | MRD− CR (1) | 27.4§ | Gr 2 | No | Cytopenias requiring support |
| 6 | M, 18 | Burkitt | Yes | BEAM | RIC | No | No | 6 | Stage IV | No (ECOG 3) | 1 × 107 TNC/m2 (Flu/Cy) | N/A | N/A | N/A | N/A | Death from pulmonary embolus |
| 7 | M, 47 | B-ALL | No, MRD+ | No | MAC | No | Yes | 4 | BM: MRD− Occult extra-medullary | Yes | 1 × 107 TNC/m2 (Flu/Cy) | MRD− CR (1) | 9.2 | Gr 2 | No | Cytopenias requiring support |
| 8 | M, 30 | B-ALL | No | No | MAC | No | Yes | 5 | MRD+ | Yes | 1 × 107 TNC/m2 (Flu/Cy) | MRD− CR (1) | 23.2§ | No | No | CAR T malignancy Cytopenias requiring support |
| 9 | M, 20 | B-ALL | No, MRD+ | No | (1) MAC (2) MAC | 2 | No | 8 | Cerebellar mass | No (release criteria**) | 1 × 107 cells/m2 (Flu/Cy) 5 × 107 cells/m2 (Flu/Cy) 1 × 108 cells/m2 (Flu/Cy) | CR (3) | 6.0§ | Gr 2 | No | Cytopenias requiring support CVAD sepsis Death from multiviral SIRS‖ |
| 10 | F, 62 | B-ALL | No | No | RIC | No | No | 4 | Extra-medullary | Yes | 1 × 107 cells/m2 (Flu/Cy) | CR (1) | 15.6§ | No | No | Cytopenias requiring support |
allo, allogeneic HSCT; auto, autologous HSCT; BEAM, carmustine, etoposide, cytarabine, and melphalan; blin, blinatumomab; BM, bone marrow; Burkitt, Burkitt lymphoma; cGVHD, chronic graft-versus-host disease; CR, complete remission; CRS, cytokine release syndrome; CVAD, central venous access device; Cy, cyclophosphamide; DLBCL, diffuse large B cell lymphoma; DLI, donor-lymphocyte infusion; ECOG, Eastern Cooperative Oncology Group; F, female; Flu, fludarabine; GI, gastrointestinal; Gr, grade; ICANS, immune effector cell-associated neurotoxicity syndrome; IFI, invasive fungal infection; M, male; MAC, myeloablative conditioning; MRD, minimal residual disease; N/A, not applicable; PD, progressive disease; RIC, reduced intensity conditioning; SIRS, systemic inflammatory response syndrome; TNC, total nucleated cell.
B-ALL response criteria: CR, <5% bone marrow blasts, negative PET-CT scan for extramedullary disease, negative magnetic resonance imaging (MRI) for central nervous system disease; MRD− CR, absence of bone marrow MRD based on molecular testing with a limit of detection of 0.005% to 0.001%. Lymphoma response was graded according to the Lugano classification.25
CRS graded according to Lee 2014 criteria.16
ICANS graded according to the CARTOX Working Group guidelines.26
Response ongoing at last follow-up.
CAR T cell–related death.
Patient 5 developed grade 2 CRS with the initial dose of CAR19 T cells and received a repeat dose of 1 × 107 TNC/m2 before escalating to the higher dose levels.
Fludarabine was omitted at the highest cell dose for patient 5 due to persistent cytopenias.
Failure of autonomous proliferation positive control, although the product itself showed no autonomous proliferation.
CAR19 T-cell products were generated with piggyBac in 15 days (n = 9) or 23 days (n = 1) and contained a median of 72.5% CAR19 T cells (range, 38.7% to 92.9%) (supplemental Figure 2; supplemental Methods). Most CAR19 T cells had CD62L−CD45RA− effector memory phenotype (80.0% ± 7.1%; mean plus or minus standard deviation), and fewer had CD62L+CD45RA− central memory phenotype (17.6% ± 6.0%). Many expressed the inhibitory marker TIM3 (55.8% ± 17.9%). Description of integration sites is detailed elsewhere (Micklethwaite et al15) but only 7% of such sites occurred within cancer-related genes and were not different to those previously described for piggyBac or viral vectors.
Nine patients survived ≥28 days and were evaluable for response (Figure 1B), with a median follow-up of 18.0 months (range, 6.0-29.2 months). The complete remission (CR) rate was 100% (example shown in supplemental Figure 3). Two patients underwent a second allogeneic HSCT while in sustained CR. At cutoff, 5 patients remained in CR of B-cell malignancy (longest, 27.4 months ongoing). Overall survival ranged from 6.0 to 29.2 months ongoing (median not reached).
Four patients relapsed, each with undetectable CAR19 T cells (median, 7.2 months). Two were eligible to receive further escalating CAR19 T-cell doses postrelapse, but did not respond. One developed CD19− B cell acute lymphoblastic leukemia (B-ALL); the other lost donor marrow chimerism and may have had allorejection of donor-derived CAR19 T cells.
Two patients developed CAR19 T-cell lymphoma after achieving CR of B-cell malignancy. In each case, the diagnosis was based on identification of a new mass composed of monoclonal CAR19 T cells (according to T-cell receptor variable β chain analysis) with abnormal phenotype, which continued to increase in size and metabolic activity in the absence of residual CD19 antigen (Figure 1C; see Micklethwaite et al15 for detailed analysis). This was first detected in patient 2 on a positron emission tomography–computed tomography (PET-CT) scan at 3.2 months, but the diagnosis was only established at 15.0 months, after multiple nondiagnostic biopsies. Treatment with cyclophosphamide, vincristine, and prednisolone led to transient response, but complications of sepsis and multiorgan failure resulted in death at 18.0 months. Surviving patients subsequently underwent PET-CT screening; patient 8 was also confirmed to have CAR19 T-cell lymphoma at 11.5 months. CR was induced with 4 cycles of augmented cyclophosphamide, doxorubicin or etoposide, vincristine, and prednisolone (CHOP). He proceeded to a second allogeneic HSCT at 16.9 months and remains in remission of both B-ALL and the CAR19 T cell lymphoma at 23.2 months.
Other adverse events are summarized in Table 1. Five deaths occurred, including 2 treatment-related deaths and 2 from relapsed B-ALL. Patient 6 died on day 3 of treatment from pulmonary embolus secondary to extensive Burkitt lymphoma surrounding abdominal vessels. Four patients with high disease burden developed cytokine release syndrome (CRS) of grade ≤2,16 with elevated serum cytokines (supplemental Figure 4). Patient 2 developed exacerbation of pre-existing chronic graft-versus-host disease (GVHD) of the skin, managed with prednisone and ibrutinib. There was no immune effector cell–associated neurotoxicity syndrome (ICANS), tumor lysis syndrome, new GVHD, or early dose-limiting toxicity.
CAR19 T cells expanded in peripheral blood of all evaluable patients (Figure 1D). Following the first infusion, CAR19 T cells peaked at a median of 16.4 CAR19 T cells per μL (range, 0.9-1824) after a median of 16 days (range, 8-24 days). Greater CAR19 T-cell expansion was noted with a high disease burden, a high percentage of CAR19 T cells in the product, and the development of CRS (supplemental Figure 5). After 1 infusion, CAR19 T cells were detectable in peripheral blood for up to 4.9 months. Patient 9, who had 3 escalating doses, had continuously detectable CAR19 T cells until his death at 6.0 months, representing the longest period seen in patients not developing CAR19 T-cell lymphoma.
In this first-in-human phase 1 clinical trial, piggyBac CAR19 T cells generated from HLA-matched sibling allogeneic donors induced CR, some sustained, in all evaluable patients with relapsed and refractory CD19+ malignancy following HSCT. However, 2 patients developed CAR19 T-cell lymphoma, raising concern about the safety of the piggyBac CAR19 T-cell production methodology (see Micklethwaite et al15).
Like other 4-1BB–based autologous products generated with viral vectors, piggyBac CAR19 T cells expanded in proportion to disease burden, persisted for months, and effectively induced minimal residual disease–negative (MRD−) CR of B-ALL.4-6 Similarly, patients with high disease burden receiving piggyBac CAR19 T cells developed CRS that was associated with elevation in cytokines but that responded to tocilizumab and dexamethasone.16,17
We observed no ICANS or CRS grade >2. This may be a result of the intrapatient dose-escalation strategy intended to avoid large CAR T-cell doses in the presence of high disease burden, a situation known to be associated with development of severe CRS and ICANS.17,18 All patients with B-ALL outside of the central nervous system in this study achieved MRD− remission after the smallest dose of piggyBac CAR19 T cells, but 4 patients subsequently relapsed. The utility of repeat escalated CAR19 T-cell dosing remains unclear.
CAR19 T cell malignancy has not previously been documented following administration of CAR T cells produced using viral vectors, other transposon systems, or piggyBac.1-6,10,11,19,20 This led to the death of 1 patient in our study; however, the second patient, who remains in CR, was responsive to standard T-cell lymphoma management. Potential drivers of malignant transformation include CAR overexpression with basal activation, prolonged stimulation through the CAR or endogenous T-cell receptor leading to secondary mutational events, or transgene insertional mutagenesis. Investigations of the pathogenesis performed to date (described by Micklethwaite et al15) do not demonstrate classical insertional mutagenesis as the cause,21 with the pattern of integration of the CAR transgene at genomic sites by piggyBac consistent with previous reports, and not appreciably different to that seen with γ-retroviral and lentiviral vectors.22-24
With this first cohort of human subjects, we demonstrate that allogeneic piggyBac CAR19 T cells administered post-HSCT achieve the efficacy seen with CAR T cells generated using viral vectors. However, recruitment to trials of piggyBac CAR19 T cells at our center has been voluntarily suspended while further investigations into the pathogenesis of CAR19 T-cell lymphoma take place. Prevention of future malignant events will require changes to the production process, with animal safety testing to provide confidence before contemplating resumption of trials. The ability of piggyBac to integrate a large amount of genetic material, and the absence of a requirement for detection of competent retrovirus or lentivirus in the final product, remain attractive characteristics of this system. Determining the cause of the malignant transformation we have observed will be key to resolving whether it has a future place in human trials.
Acknowledgments
The authors acknowledge the patients and transplant donors who participated in this study. Donor venesection was performed at Australian Red Cross Lifeblood under the direction of Philip Mondy, Elizabeth Knight, and Justine O’Donovan.
This work was supported by the Priority-driven Collaborative Cancer Research Scheme and was also funded by the Cure Cancer Australia Foundation and Cancer Australia (grant 1047454), the National Health and Medical Research Council (grant 1102172), Cancer Council New South Wales (translational program grant #TPG 19-01), and the Sydney West Translational Cancer Research Centre, which was funded by Cancer Institute NSW (15/TRC101). D.C.B. was supported by a Leukaemia Foundation of Australia Clinical Scholarship, and a Haematology Society of Australia and New Zealand New Investigator Scholarship. The Australian governments fund Australian Red Cross Lifeblood to provide blood, blood products, and services to the Australian community.
Flow cytometry was performed at the Westmead Scientific Platforms, which were supported by the Westmead Research Hub, Cancer Institute NSW, the National Health and Medical Research Council, and the Ian Potter Foundation.
Donor apheresis was performed at The Children’s Hospital at Westmead.
Authorship
Contribution: K.P.M., D.J.G., and E.B. conceptualized the study; K.P.M., D.C.B., and L.E.C. were responsible for study methodology; D.C.B., G.S., J.A.S., L.M., E.A., K.M., J.B., G. Mathew, G. McCaughan, H.M.M., R.S., K.L., P.J.S., K.P.M., E.B., B.S.G., V.A., and D.O.I. were responsible for investigation; D.C.B., G.S., K.L., H.M.M., and W.J. were responsible for formal analysis; L.E.C. and S.A. were responsible for validation; D.C.B. wrote the original draft; D.C.B., K.P.M., E.B., and D.J.G. wrote, reviewed, and edited the manuscript and acquired funding; and K.P.M., E.B., L.E.C., D.J.G., P.J.S., T.A.O., and V.A. provided supervision.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
The current affiliations for G. McCaughan are Department of Haematology and Bone Marrow Transplantation, St Vincent’s Hospital Sydney, Darlinghurst, NSW, Australia; and St Vincent’s Clinical School, UNSW Medicine, The University of New South Wales, Sydney, NSW, Australia.
Correspondence: Kenneth P. Micklethwaite, Department of Haematology, Westmead Hospital, Hawkesbury Rd, Westmead NSW 2145, Australia; e-mail: kenneth.micklethwaite@sydney.edu.au.
Data will be provided on request via e-mail to the corresponding author.
The online version of this article contains a data supplement.
There is a Blood Commentary on this article in this issue.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal