

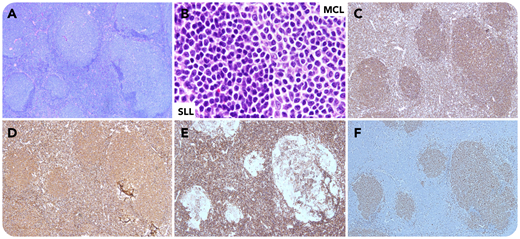
A 57-year-old man with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and no prior therapy, presented with lymphadenopathy and white blood cell count of 275.2 × 109/L. A lymph node biopsy showed nodular infiltrates of centrocyte-like cells and diffuse small lymphocytes (panels A and B; hematoxylin and eosin stain, 4× and 100× objective; original magnification, ×40 and ×1000, respectively). The small lymphocytes were CD79adim+, CD5+, CD23+, and cyclin D1−; the nodular infiltrates were CD79abright+, CD5+, CD23−, and cyclin D1+ (panels C-F, respectively; 4× objective; original magnification ×40). Flow cytometry detected 2 B-cell populations: one was CD20dim+, CD38−, and κ+, and the other was CD20bright+, CD38+, and λ+. Cytogenetics detected 2 distinct clones: one with trisomy 12 and del(13)(q14), and the other with t(11;14)(q13;q32). Polymerase chain reaction revealed 2 distinct clones, one with an IgH rearrangement identical with the original CLL and the other with a different rearrangement. Findings were diagnostic of composite lymphoma (CL): mantle cell lymphoma (MCL) and SLL. The patient was followed up with expectant management and no new treatment was initiated.
CL is the cooccurrence of 2 distinct lymphomas: both non-Hodgkin lymphomas (NHLs) or an NHL and a Hodgkin lymphoma. Composite MCL and CLL/SLL is very rare. The 2 components in our patient were clonally unrelated, suggesting 2 distinct disease processes. A multiparametric approach is necessary to diagnose CL, which can have significant therapeutic and prognostic implications.
A 57-year-old man with chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and no prior therapy, presented with lymphadenopathy and white blood cell count of 275.2 × 109/L. A lymph node biopsy showed nodular infiltrates of centrocyte-like cells and diffuse small lymphocytes (panels A and B; hematoxylin and eosin stain, 4× and 100× objective; original magnification, ×40 and ×1000, respectively). The small lymphocytes were CD79adim+, CD5+, CD23+, and cyclin D1−; the nodular infiltrates were CD79abright+, CD5+, CD23−, and cyclin D1+ (panels C-F, respectively; 4× objective; original magnification ×40). Flow cytometry detected 2 B-cell populations: one was CD20dim+, CD38−, and κ+, and the other was CD20bright+, CD38+, and λ+. Cytogenetics detected 2 distinct clones: one with trisomy 12 and del(13)(q14), and the other with t(11;14)(q13;q32). Polymerase chain reaction revealed 2 distinct clones, one with an IgH rearrangement identical with the original CLL and the other with a different rearrangement. Findings were diagnostic of composite lymphoma (CL): mantle cell lymphoma (MCL) and SLL. The patient was followed up with expectant management and no new treatment was initiated.
CL is the cooccurrence of 2 distinct lymphomas: both non-Hodgkin lymphomas (NHLs) or an NHL and a Hodgkin lymphoma. Composite MCL and CLL/SLL is very rare. The 2 components in our patient were clonally unrelated, suggesting 2 distinct disease processes. A multiparametric approach is necessary to diagnose CL, which can have significant therapeutic and prognostic implications.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal