


Abstract
Although therapeutic strategies have been adapted to age and comorbidities for a long time, almost all multiple myeloma (MM) patients currently receive similar treatment, whatever their disease risk category. However, high-risk MM patients still constitute an unmet medical need and should benefit from the most efficient drug combinations. Herein, we review and discuss how to optimally define risk and why a revision of the current definition is urgently needed.
Introduction
Multiple myeloma (MM) survival has improved dramatically in last decade. However, although some patients experience long remission and even cure in rare cases, prognosis is still poor for high-risk patients, which remains an unmet medical need. At the same time, the prognostic factors have also changed as a result of technological advances providing new data and because some of the novel drugs have changed the disease course. So the question is: Who are the real high-risk MM patients in 2020? Here, we review the most recent data about MM risk factors and discuss why the current definition needs revision. The stakes are high because after decades of treatment only adapted to age and renal function, the time has probably come to also adapt it to the risk.
Multiple prognostic factors in myeloma
MM is probably the cancer with the most number of prognostic parameters described.1 Different categories can be distinguished: factors related to patients, tumor load, and intrinsic cellular features, as well as mixed factors. In the first category, age is a crucial factor because of its associated comorbidities and performance index,2 also dictating eligibility for therapeutic intensification.3,4 Factors related to tumor load are anemia, thrombocytopenia, elevated serum β2-microglobulin, and lactate dehydrogenase levels. Cytogenetic and molecular abnormalities belong to the category of factors related to the intrinsic cellular characteristics of the tumor, along with high plasma cell proliferation index,5 as well as leukemic presentation and extramedullary disease.6-8 Finally, some poor prognosis factors are linked to patient and tumor, such as hypoalbuminemia, renal failure, and poor response to treatment. Among all prognostic factors, genetic abnormalities and response to treatment are the most robust.
The weight of genes
MM is complex and heterogeneous for genetic abnormalities.9-11 It is complex because its development and progression are induced by multiple genomic events, and it is heterogeneous because the recurrence of the same molecular abnormalities is low, and as several subclones evolve differently within the same individual. Even if the cause and effect relationship is probably not linear, this undoubtedly contributes to the wide prognostic disparities in MM. In practice, we need to remember that conventional karyotype is not recommended for genomic analysis in MM and that plasma cell sorting is mandatory, whatever the analysis performed (fluorescence in situ hybridization [FISH], single nucleotide polymorphism array, or next-generation sequencing [NGS]).
Prognostic cytogenetic abnormalities
The most common cytogenetic abnormality is hyperdiploidy, which is present in 55% of patients. The trisomies, preferentially affecting the odd chromosomes (3, 5, 7, 9, 11, 15, 19, and 21), are generally associated with a rather favorable prognosis, but the reality is more complex and depends on the exact chromosomes involved: for instance, data suggest that only trisomies 3 and 5 have a real favorable impact on overall survival but, conversely, trisomy 21 is associated with an unfavorable prognosis.12
The second abnormality in terms of frequency affects the 14q32 region, which is altered in 45% to 50% of patients in the form of translocations and involves the locus of the immunoglobulin heavy chains (IGH). The most frequent is t(11;14), which is found in 20% of patients and leads to hyperexpression of cyclin D1. It does not have any prognostic implications at the moment, but its detection is interesting because it correlates with an increased sensitivity to venetoclax, a BCL2 inhibitor.13-15 The second most common is t(4;14), which is found in 12% to 15% of patients. Specific to MM, it has the particularity of deregulating 2 genes, FGFR3 and NSD2, with the latter being responsible for its prognostic impact. t(4;14) is associated with an unfavorable prognosis, but several elements must be taken into account for its accurate interpretation. First, some concomitant factors, such as 1p32 deletion,16 can considerably worsen its prognostic value. In addition, various clinical data have suggested that bortezomib is of particular interest in patients with t(4;14).17-19 The widespread use of this drug has probably contributed to reducing the unfavorable prognosis of that translocation. Finally, a subgroup of t(4;14) seems to confer a poor prognosis, whereas others seem neutral (the only ones really abrogated by bortezomib?). A molecular dissection of this abnormality is ongoing. Other recurrent translocations have been described at a much lower frequency (<3.5%), in particular t(14;16) implicating cMAF. A Mayo Clinic study conducted in 2003 showed a negative impact of t(14;16) on survival in 15 patients. The Intergroupe Francophone du Myélome (IFM) failed to find a significant difference in survival.20 A recent study analyzed 223 patients possessing t(14;16), the largest cohort to date, but an independent prognostic value was not demonstrated.21 Despite these contradictory data, t(14;16) is included in the revised-International Staging System (R-ISS) as carrying a poor prognosis.22
Other prognostic abnormalities considered secondary are frequently found. The gain of the long arm of chromosome 1 is present in one third of newly diagnosed MM (NDMM). Its molecular target(s) remains unknown, although most of the studies have focused on CKS1B (1q21). The actual prognostic value of 1q gain is still debated, because some recent data suggest that only an amplification (>3 copies) would be of high risk, particularly in the background of ISS-3,23,24 but this will have to be confirmed in prospective studies. Another secondary abnormality associated with an unfavorable prognosis is the 1p32 deletion, targeting FAF1 and CDKN2C. It is unknown which of these 2 genes is the primary target of the deletion. del(1p32) is observed in 8% of NDMM cases and has a prognostic impact almost identical to del(17p).25
Finally, deletion of the short arm of chromosome 17 is undoubtedly the most potent prognostic factor in MM. Although unanimously recognized, some questions are still debated. The first concerns the prognostic threshold for clone size, leading to confusing data about the ability of new drugs to abrogate the impact of del(17p). Recently a meta-analysis of European data including >1000 patients with del(17p) with variable clone size was performed, confirming previous data from the IFM,26 with a significant clinical impact of the subclonality value of 55% to 60% by FISH.27 The practical consequence is the need to quantify any del(17p) by FISH. With this threshold, del(17p) is observed in 8% of NDMM cases. The second question addresses its molecular target; most studies have focused on TP53, localized in the minimal deleted region; however, the fact that the remaining allele is mutated in only a third of cases (unlike chronic lymphoid leukemia)28 is surprising. A third question concerns the mono- or biallelic nature of the abnormality. Indeed, recent data suggest that only patients with a “double-hit” biallelic inactivation of TP53 (del/mut most of the time) are at high risk.23 In contrast, we have recently demonstrated in a large cohort of homogeneously treated NDMM patients that, even if an isolated del(17p) is less dire than a double hit, it is clearly a poor prognostic factor in MM.29
What about the prognostic impact of the mutations?
Since 2012, several publications have reported the use of NGS in MM, confirming the huge molecular heterogeneity; there are many mutations, and few are recurrent. The most frequently mutated genes are KRAS and NRAS (20-25% of NDMM cases), followed by DIS3, BRAF, and FAM46C (∼10% of NDMM cases). All other genes are mutated in <10% of patients. Some studies have addressed the prognostic value of these mutations but with a median follow-up that remains relatively short until now. TP53 mutation, which is observed in 5% to 6% of NDMM cases, is the only 1 consistently found to be associated with shorter survival.30 With a longer follow-up on large homogeneous cohorts allowing a robust analysis of the subgroups, other prognostic mutations may be highlighted in the future.
Beyond the nature of mutated genes, the mutation burden and signature are also important. For instance, a good-risk group including 18% of NDMM patients has recently been identified; in addition to chromosome 9 gain, they display a lower mutation burden and a profile driven by an age-related signature.31
Toward a multiparameter definition of the cytogenetic risk of MM
The International Myeloma Working Group recommends the detection of t(4;14), t(14;16), and del(17p) to define high-risk MM.3 These 3 abnormalities are taken into account in the R-ISS score,22 which is also based on the serum lactate dehydrogenase level, along with the serum β2-microglobulin and albumin levels that made up the original International Staging System.32 However, this definition now seems oversimplified and too restrictive, and it may lead to misclassification because it is only based on 3 unweighted cytogenetic abnormalities, mixed with biochemical factors. Co-occurrence and clonality significantly affect the importance of each of the current risk factors. The IFM performed a multivariate analysis of 1200 patients by single nucleotide polymorphism array and FISH. Five abnormalities associated with a shorter overall survival were identified: del(17p), del(1p32), gain 1q, t(4;14), and trisomy 21. The only protective abnormality was trisomy 5. A prognostic score including these 6 variables was developed; each was associated with a specific prognostic value (Table 1).33 Its ability to detect 3 prognostic groups has been validated in a cohort of patients treated with the most modern first-line therapeutic approaches (Figure 1), and it outperformed R-ISS. t(14;16) was available for only 1 data set; it did not show any significant prognostic impact. Of note, the most frequent co-occurrence was trisomies 5 and 21, followed by 1q gain among patients with t(4;14) and del(1p32).33 In clinical practice, this score may help to identify “true” high-risk t(4;14), pending molecular dissection. The search for the 6 abnormalities can be carried out in any laboratory in which plasma cell sorting and FISH are available. Nevertheless, targeted NGS approaches allow the assessment of all copy numbers variations, IGH translocations, and recurrent mutations in 1 technique.34
Weighted cytogenetic prognosis factors in MM
| Cytogenetic factor | Coefficient |
|---|---|
| Trisomy 5 | −0.3 |
| Trisomy 21 | 0.3 |
| t(4;14) | 0.4 |
| Gain 1q | 0.5 |
| del(1p32) | 0.8 |
| del(17p) | 1.2 |
| Risk (scote = sum of coefficients) | |
| Low | ≤0 |
| Intermediate | >0 and ≤1 |
| High | >1 |
| Cytogenetic factor | Coefficient |
|---|---|
| Trisomy 5 | −0.3 |
| Trisomy 21 | 0.3 |
| t(4;14) | 0.4 |
| Gain 1q | 0.5 |
| del(1p32) | 0.8 |
| del(17p) | 1.2 |
| Risk (scote = sum of coefficients) | |
| Low | ≤0 |
| Intermediate | >0 and ≤1 |
| High | >1 |
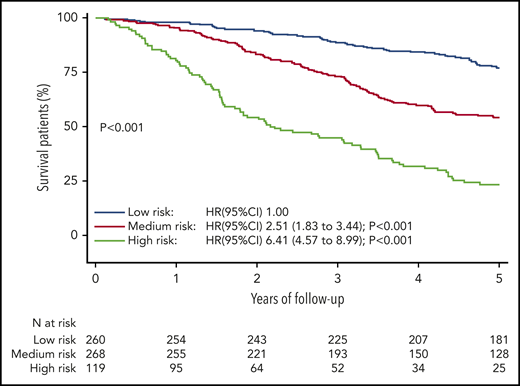
Overall survival according to the 3 risk categories defined by the IFM score in the training cohort. CI, confidence interval; HR, hazard ratio. Reprinted from Corre et al35 with permission.
Overall survival according to the 3 risk categories defined by the IFM score in the training cohort. CI, confidence interval; HR, hazard ratio. Reprinted from Corre et al35 with permission.
The importance of the response to treatment: “risk is a dynamic concept”
Response to treatment is a major prognostic factor for MM. Fifteen years ago, Durie et al were the first to show that the underlying dominant predictor for survival is time to progression, ahead of depth of response.36 The Mayo Clinic was the first to specifically describe the adverse prognostic impact of an early relapse after intensive strategy.37 Despite the current availability of effective salvage treatments, an IFM study recently showed that early relapse after an intensive first-line therapy still negatively impacts survival.35 Interestingly, approximately two thirds of early relapsing patients were not initially considered high risk.
Significant progress has recently been made in assessing the depth of response thanks to the development of sensitive techniques to determine the level of minimal residual disease (MRD). Indeed, next-generation flow and NGS permit achievement of the unprecedented sensitivity threshold of 1 tumor plasma cell in 1 million (10−6) analyzed bone marrow cells. Achieving an undetectable MRD is associated with significantly longer progression-free and overall survival, whether in the first line or at relapse.38 As deep as it is, the nondetectability of MRD must be sustained over time to be of optimal quality. Importantly, obtaining an undetectable MRD may abrogate some high-risk cytogenetic factors; conversely, a standard-risk subject with a positive MRD may switch to the high-risk group.39,40 This shows that risk is a dynamic concept; the reality is that we probably miss the prognostic impact of clonal architecture, epigenetics, immune microenvironment, and many other features that we do not take into account for lack of sufficient knowledge.
When faced with a high-risk patient, it is imperative to opt for the therapeutic strategy most likely to achieve a sustained undetectable MRD (<10−6). If MRD remains positive, an early therapeutic intervention may be necessary.
Conclusions
Despite the considerable enrichment of the therapeutic arsenal, high-risk MM still constitutes an unmet medical need in 2020. Double transplant, chimeric antigen receptor T cells, T-cell engagers… What are the most effective therapeutic strategies for these patients? This is another question that we have to address as soon as possible. The definition of risk evolves with the arrival of new treatments. Hopefully, the next 2 decades will be as prolific as the past few. The time has come to readdress the risk stratification, keeping in mind that risk evolves over the course of the disease, that risk factors may co-occur and alter the impact of each other, and that therapy may affect the importance of each of the risk factors individually and as a group. We believe that the use of a multiparametric cytogenetic score, such as the one proposed by the IFM, is a valuable option to assess risk in clinical practice. Evaluation of the MRD allows for adjustments to be made if necessary.
Acknowledgment
The Centre de Recherches en Cancérologie de Toulouse Team 13 is supported by Fondation Association pour la Recherche sur le Cancer (ARC) grant PGA1*20160203788.
Authorship
Contribution: J.C., N.C.M., and H.A.-L. wrote the manuscript.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Hervé Avet-Loiseau, Unit for Genomics in Myeloma, Institut Universitaire du Cancer–Oncopole, 1 Avenue Irène Joliot-Curie, 31100 Toulouse, France; e-mail: avetloiseau.herve@iuct-oncopole.fr.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal