

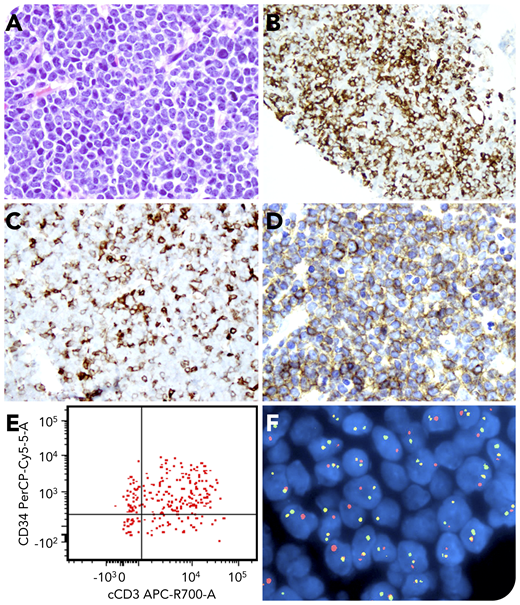
A 43-year-old man was diagnosed with Ph+ chronic myeloid leukemia (CML) in 2017 and was prescribed tyrosine kinase inhibitor therapy with suboptimal compliance. In January 2020, he had 22% aberrant myeloid blasts in his peripheral blood (only 3% to 5% blasts in bone marrow). Therapy with dasatinib was initiated, but he was lost to follow-up. A few weeks later, he presented with abdominal pain, and a 4 × 3.6-cm retroperitoneal soft tissue mass was found on a computed tomographic scan. Hematoxylin and eosin staining of the mass showed sheets of atypical, medium-sized blasts with a high nucleus/cytoplasm ratio (panel A; original magnification ×400). These blasts were partially positive for CD34 (panel B; original magnification ×200); dimly and partially positive for CD117 (panel C; original magnification ×200), CD3 (not shown), CD33 (panel D; original magnification ×400), and GATA3 (not shown); but negative for myelomonocytic, B- and T-cell antigens, including CD1a, CD2, CD4, CD5, CD7, CD8, and TdT. Limited flow cytometry showed that the blasts were positive for cytoplasmic CD3 (panel E). Fluorescence in situ hybridization showed that 91% of the blasts harbored the BCR-ABL1 fusion (panel F, yellow signals; original magnification ×1000). There was no monoclonal TCR-γ gene rearrangement.
The overall findings were most consistent with early T-cell precursor acute lymphoblastic leukemia (ETP-ALL). This case is only the second documented ETP-ALL as a blast crisis of CML, but it is the first one in which the ETP-ALL blast crisis was extramedullary.
A 43-year-old man was diagnosed with Ph+ chronic myeloid leukemia (CML) in 2017 and was prescribed tyrosine kinase inhibitor therapy with suboptimal compliance. In January 2020, he had 22% aberrant myeloid blasts in his peripheral blood (only 3% to 5% blasts in bone marrow). Therapy with dasatinib was initiated, but he was lost to follow-up. A few weeks later, he presented with abdominal pain, and a 4 × 3.6-cm retroperitoneal soft tissue mass was found on a computed tomographic scan. Hematoxylin and eosin staining of the mass showed sheets of atypical, medium-sized blasts with a high nucleus/cytoplasm ratio (panel A; original magnification ×400). These blasts were partially positive for CD34 (panel B; original magnification ×200); dimly and partially positive for CD117 (panel C; original magnification ×200), CD3 (not shown), CD33 (panel D; original magnification ×400), and GATA3 (not shown); but negative for myelomonocytic, B- and T-cell antigens, including CD1a, CD2, CD4, CD5, CD7, CD8, and TdT. Limited flow cytometry showed that the blasts were positive for cytoplasmic CD3 (panel E). Fluorescence in situ hybridization showed that 91% of the blasts harbored the BCR-ABL1 fusion (panel F, yellow signals; original magnification ×1000). There was no monoclonal TCR-γ gene rearrangement.
The overall findings were most consistent with early T-cell precursor acute lymphoblastic leukemia (ETP-ALL). This case is only the second documented ETP-ALL as a blast crisis of CML, but it is the first one in which the ETP-ALL blast crisis was extramedullary.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal