

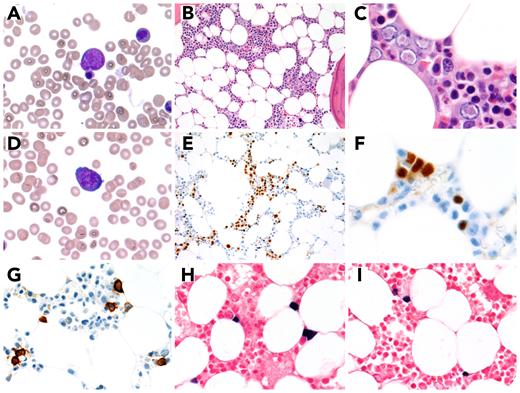
A 55-year-old man with a history of κ light-chain plasma cell myeloma, in remission and undergoing therapy (lenalidomide, bortezomib, dexamethasone, and zoledronic acid), presented for routine bone marrow follow-up. The complete blood count showed normal hemoglobin/hematocrit (13.3 g/dL; 40.0%) with leukopenia (2860 white blood cells per microliter) and thrombocytopenia (59 000 platelets per microliter). Bone marrow examination showed large left-shifted erythroid precursors with prominent intranuclear inclusions on aspirate (panels A,D; Wright stain; original magnification ×1000) and biopsy (panels B-C; hematoxylin and eosin stain; original magnification ×200 and ×500, respectively). Parvovirus immunohistochemistry was positive (panels E-F; original magnification ×200 and ×500, respectively). No significant morphologic abnormalities were seen in the granulocytic or megakaryocytic lineages. Subsequent polymerase chain reaction analysis was positive for parvovirus B19. CD138 immunohistochemical-stained <5% plasma cells (panel G; original magnification ×500) with polytypic κ and λ in-situ hybridization studies (panels H-I; original magnification ×500). Concurrent flow cytometry was negative for minimal residual disease, confirming continued remission of myeloma.
Parvovirus is associated with pure red cell aplasia and anemia in immunocompromised patients, such as patients undergoing chemotherapy. This patient’s presentation is atypical, because he presented with normal hemoglobin and hematocrit values. Further evaluations were pursued because of classic histologic findings. The patient’s physician instituted monitoring of the patient’s parvovirus infection, and he subsequently received IV immunoglobulin.
A 55-year-old man with a history of κ light-chain plasma cell myeloma, in remission and undergoing therapy (lenalidomide, bortezomib, dexamethasone, and zoledronic acid), presented for routine bone marrow follow-up. The complete blood count showed normal hemoglobin/hematocrit (13.3 g/dL; 40.0%) with leukopenia (2860 white blood cells per microliter) and thrombocytopenia (59 000 platelets per microliter). Bone marrow examination showed large left-shifted erythroid precursors with prominent intranuclear inclusions on aspirate (panels A,D; Wright stain; original magnification ×1000) and biopsy (panels B-C; hematoxylin and eosin stain; original magnification ×200 and ×500, respectively). Parvovirus immunohistochemistry was positive (panels E-F; original magnification ×200 and ×500, respectively). No significant morphologic abnormalities were seen in the granulocytic or megakaryocytic lineages. Subsequent polymerase chain reaction analysis was positive for parvovirus B19. CD138 immunohistochemical-stained <5% plasma cells (panel G; original magnification ×500) with polytypic κ and λ in-situ hybridization studies (panels H-I; original magnification ×500). Concurrent flow cytometry was negative for minimal residual disease, confirming continued remission of myeloma.
Parvovirus is associated with pure red cell aplasia and anemia in immunocompromised patients, such as patients undergoing chemotherapy. This patient’s presentation is atypical, because he presented with normal hemoglobin and hematocrit values. Further evaluations were pursued because of classic histologic findings. The patient’s physician instituted monitoring of the patient’s parvovirus infection, and he subsequently received IV immunoglobulin.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal