

Introductions
Immune thrombocytopenia (ITP) is an acquired thrombocytopenia caused by immune-mediated platelet destruction and impaired platelet production. As the immunosuppressive therapy, high-dose dexamethasone (HD-DXM) has been recommended as the standard first-line treatment. Nevertheless, approximately half of ITP patients relapse within 6 months and require further therapies. All-trans retinoic acid (ATRA) is a derivative of vitamin A that has an immunomodulatory effect on hemopoiesis. Our previous study demonstrated that ATRA could induce a more rapid and long-lasting response in patients with corticosteroid-resistant or relapsed ITP (Lancet haematology, 2017). In addition, we found that ATRA corrected impaired platelet production by regulating the complement-IL-1β loop and TNFAIP3/NF-κB/SMAD7 signaling pathway in ITP (Br J Haematol, 2018; Haematologica, 2019). These findings suggested that the addition of ATRA to HD-DXM in treatment-naive patients could improve sustained response rate based on the synergetic function. Here, we present the results of the first prospective, multicenter, randomized, controlled trial with the largest cohort to date comparing the efficacy and safety of HD-DXM plus ATRA vs HD-DXM as first-line therapy in newly diagnosed adult primary ITP patients.
Methods
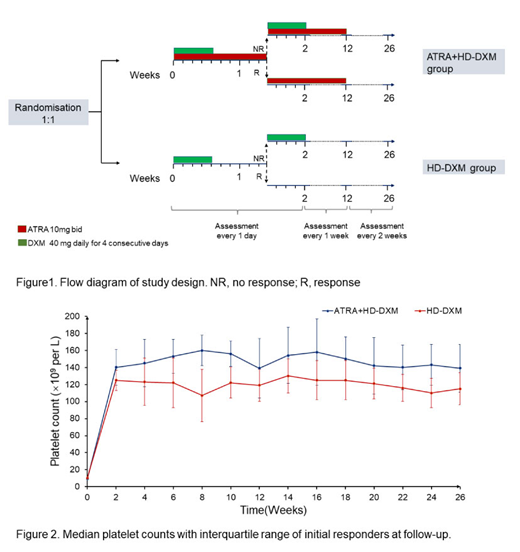
In this open-label, randomized, phase 2 trial, we enrolled adult ITP patients from 6 different tertiary medical centers in China. Eligible subjects had confirmed newly-diagnosed, treatment-naive ITP; platelet counts <30×109/L or platelet counts < 50×109/L and significant bleeding symptoms (WHO bleeding scale 2 or above).Eligible patients were randomly assigned 1:1 with an interactive web-based response system to receive either oral ATRA (10 mg twice daily) plus HD-DXM or HD-DXM monotherapy for 12 weeks. DXM was administered orally at 40 mg daily for 4 consecutive days to both arms. The 4-day course of dexamethasone was repeated on days 11 to 14 in the case of lack of response by day 10(Figure 1). The primary endpoint was 6-month sustained response (SR) defined as platelet counts maintained > 50×109/L without any additional ITP-modifying therapy at the 6-month follow up. Key secondary endpoints were initial response by day 14 (OR: platelet count ≥30×109/L and at least 2-fold increase of the baseline platelet count and absence of bleeding; CR: platelet count ≥100×109/L), duration of response (DOR), bleeding scores, and adverse events (AEs).
Results
Between June 2015, and July 2018, 300 patients were randomly allocated into either ATRA plus HD-DXM (n=150) or HD-DXM monotherapy (n=150). At the 6-month follow-up, the proportion of patients with SR was significantly higher in the ATRA plus HD-DXM group than in the HD-DXM monotherapy group (61% vs 37%, p= 0.009). So far, the increase of almost one quarter is very encouraging.
The combination of ATRA and HD-DXM resulted in a higher incidence of early OR at day 14 compared with HD-DXM monotherapy (83% vs 67%, P=0.031), and the CR rate was 60.0% (ATRA+HD-DXM) vs 40.6% (HD-DXM) (P=0.015). Throughout the follow-up period, overall DOR was greater in the combination group, estimated by the Kaplan-Meier analysis. Fewer patients in the combination group than in the monotherapy group relapsed during follow-up (p< 0.001), and the median time to relapse was 75 days (ATRA+HD-DXM) vs 48 days (HD-DXM).
Bleeding was more effectively controlled in the ATRA plus HD-DXM arm, with fewer bleeding events and lower bleeding scores. There was no difference between the 2 groups in terms of rescue treatments. All subjects tolerated the treatment well, and no grade 4 adverse events or treatment-related death were reported. No statistically significant differences were observed in the incidence of treatment-related AEs between the two groups.
Conclusions
ATRA plus HD-DXM is an effective and safe treatment for ITP as a first-line therapy that can provide a sustained prolonged response in adults. This therapy could be a new treatment option for ITP subjects.
Disclosures No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal