

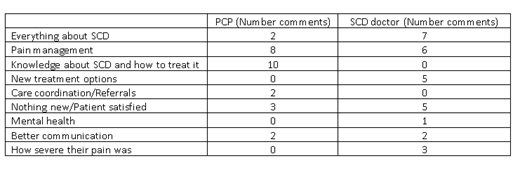
The Health Resources and Services (HRSA)-sponsored Sickle Cell Disease (SCD)Treatment Demonstration Regional Collaborative Program, EMBRACE SCD Florida has three aims: 1. To educate providers about SCD, 2. To assess patients' perception on health care and barriers encountered, and 3. To increase hydroxyurea (HU) treatment as disease-modifying therapy. We report the patients' perception on health care delivery as assessed by surveys of 65 patients at two SCD centers in South Florida. All participants signed the IRB-approved informed consent/assent and completed a 46-question survey. Surveys addressed patient demographics, HU use, pain experienced, facility utilization and confidence in SCD doctors and primary care providers (PCPs). Parents represented 62 % of the sample respondents. There were 37 female and 28 male patients, with a mean age of 14.8 years, median 12 years (range 1-45). Patients were self-identified as SS (N=42, 65%), SC (N=8), sickle-β+ thalassemia (N=5), sickle-β0 thalassemia (N=2), other (N=1), and 7 (11%) did not know their genotype. Most (55%) were African-Americans; 26% Haitians, 12% Black non-African-American or other, and 6% were White. Nine percent were Hispanic. Insurance coverage was identified as Medicaid (75%), Managed Care Organization (7%), Medicare (13%), and private insurance (5%). Of the 44 patients with SS and Sβ0, 84% (N=37) received medical advice to take HU from SCD provider. In addition, 12 patients (4 unknown type, 5 Sβ+ and 3 SC) were advised to take HU for a total of 49 or 75% of all patients surveyed. Seventy-eight percent (N=38) of those agreed to be treated, and 22% (N=11) declined HU. Eighty-four percent of those who agreed to be treated (N=32) reported taking HU as prescribed. Those patients who have received HU identified many barriers: lack of money to pay (N=5), nausea (N=5), hair loss (N=1), do not like the taste (N=8), do not like to take medications so they either do not take it frequently (N=7) or force themselves to take it (N=12), lack of effectiveness for their pain (N=10), and forgetting to take HU (N=18). Eighteen of 49 (37%) said they had no problems taking HU. We asked all patients about their pain experience. Of the 63 who responded, 30 (47.6%) said pain was managed well all the time, whereas the rest perceived difficulties in pain management: 20 (31.7%), 12 (19%), and one (1.6%) perceived their pain was managed well 75% of time, 50% of the time, and 25% or less of the time, respectively. The frequency of taking pain medications was variable among patients. The most common frequency of taking pain medications was several times a month (24 of 63 or 38%), but ranged from taking pain medication daily (N=9, 14%) to never or almost never (N=10, 16%). The emergency room (ER) was the first place they would go to when they get sick. One patient reported he prefers staying home. Patients reported a median of two ER visits (range 0-45) and two hospitalizations (range 0-30) in the previous 12 months. Almost all (92%) patients reported having a PCP. Sixty-seven percent visited the PCP 1-3 times per year, whereas 88% visited the SCD doctor 4-12 times per year. Whereas 68.3% patients trusted their PCP to manage their SCD, their level of trust with the SCD doctor was 95.2% (p <0.01). Similarly, 68% patients agreed that both the PCP and the SCD doctor should share responsibilities in their care. The table shows what participants considered most important for their PCP and their SCD doctor to know or learn about SCD. The most common single thing participants would change about the health care system was insurance/health care coverage (N=7), improved communication with providers (N=4), better care (N=2), or to have a cure for SCD (N=2). Six would not change anything. Eighty-four percent of patients did not know how to contact Sickle Cell Disease of America (SCDAA). Nine patients or parents (14%) felt discriminated against by health providers (N=3, doctors, nurses, pharmacy) and others (N=6, employers, classmates, others) as a result of their SCD. We identified five opportunities for quality improvement: 1. Improve pain control as 52.4% patients viewed their pain was sub-optimally managed, 2. Further examine and decrease barriers for HU treatment, 3. PCP education, as 31.7% of patients lacked trust in their competence, 4. Educate and encourage patient interaction with community-based organizations like SCDAA, and 5. Explore policy change in health care insurance coverage.
Alvarez:Forma Therapeutics: Consultancy; Novartis: Consultancy. Clay:Novartis: Speakers Bureau. Black:NHLBI: Research Funding; Micelle BioPharma: Research Funding; Pfizer: Research Funding; Sancilio and Company: Research Funding; Sanofi: Consultancy; Prolong Pharmaceuticals: Consultancy; Novartis: Research Funding; HRSA: Research Funding. Osunkwo:Novartis: Consultancy, Speakers Bureau; Pfizer: Consultancy; Terumo: Speakers Bureau; Micella Biopharma: Other: DSMB member.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal