

Introduction
Acute myeloid leukemia (AML) is a highly aggressive form of leukemia with poor long-term survival. Our clinical development of a targeted radiation treatment for relapsed/refractory AML disease led to an impressive two-year overall survival (OS) rate of 41% (Stein et al., 2019) in contrast to <10% reported for similar patients (Duval et al., 2019). Unfortunately, a lack of a preclinical model for TMI has impaired further scientific advancement. Ionizing radiation therapy (RT) has been shown to have immune modulatory functions; however, previous studies demonstrated that its efficacy is limited by activation of the radiation-induced tolerogenic TLR9/IL-6/STAT3 signaling axis in myeloid immune cells (Gao et al., 2013; Won et al., 2017). TLR9+ myeloid cells (macrophages, AML, etc) can be efficiently targeted using TLR9 agonists (CpG) conjugated with oligonucleotide (ODN) drugs (e.g., siRNA) to eliminate STAT3 signaling. Such a strategy has been shown to synergize with local tumor RT to prevent tumor recurrence (Gao et al., 2013). A CPG-STAT3-dODN inhibitor (CSI) has been previously reported as an effective immunotherapy for AML (Zhang et al., 2016), but the efficacy of immunotherapeutic agents is drastically reduced at high disease burden (Pai et al., 2019). Therefore, we hypothesized that the immunomodulatory effects of low dose RT can be augmented by blocking the STAT3 signaling in AML cells, enhancing the efficacy of CSI in a high-disease burden model.
Methods
We first developed a TMI treatment methodology using a Precision X-RAD small animal irradiator. A whole body CT image was acquired, and three-dimensional (3D) dose calculations were performed using a Monte Carlo dose engine-based SmART-Plan treatment system (van Hoof et al, 2013; Downes et al., 2009; Faddegon et al., 2009). Before treatment, mice were further imaged to verify target anatomy prior to delivering precise radiation doses to the entire skeletal system and spleen while sparing vital organs (lungs, liver, gut).
We used a Cbfb-MYH11/Mpl (CMM)-induced mice leukemia model. At 5-10% CMM-GFP cells in peripheral blood (~20-30% in bone marrow; high disease burden), the mice were treated with three doses of CSI (2.5mg/kg) on alternate days with or without 4 Gy radiation (TMI or total body irradiation [TBI]). Cy3 labeled CSI uptake studies were carried out 48h post RT by flow cytometry, and immune cell trafficking and activation studies were conducted by harvesting bone marrow and spleen cells on day 8 post RT.
Results
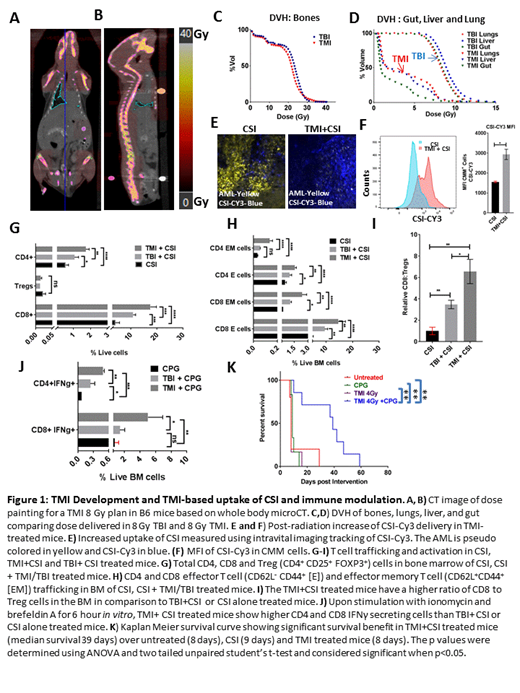
Dose volume histogram (DVH) and radiation dose painting show that the TMI treatment plan significantly reduced doses to critical organs (lungs, liver, gut) while maintianing the same dose to the skeleton and spleen, unlike TBI (same dose to entire body) (Figure 1A-D). In TMI-treated mice, the CSI-Cy3 uptake was significantly higher in CMM cells than in the CMM cells of mice treated with CSI alone, indicating improved delivery post RT (Figure 1E, F). The trafficking of T helper cells (CD4+) and cytotoxic T lymphocytes (CD8+; CTLs) as well as effector (CD62L-CD44+) and effector memory T cells (CD62L+CD44+) is significantly augmented in the bone marrow of TMI+CSI treated mice compared to levels in mice treated with TBI+CSI or CSI alone (Figure 1G, H). An increased total number of IFNγ secreting CTLs, and a higher CD8:Treg (CD4+CD25+FOXP3+) ratio indicate enhanced anti-tumerogenic activity in TMI+CSI treated mice over that of mice treated with TBI+CSI or CSI alone (Figure 1I, J). Similarly, myeloid cell trafficking and activation was augmented in TMI-treated bone marrow (data not shown). The benefit of augmented immune modulation in TMI+CSI combinatorial therapy is reflected in a significantly increased survival (~39 median survival days) over untreated mice and those treated with CSI or TMI alone ( ~8-9 days median survival) (Figure 1K).
Conclusion
This is the first report of a novel radio-immunotherapy using a systemic targeted precise RT (TMI) in combination with STAT3 down-regulation (CSI) in AML. As hypothesized, low-dose targeted RT in combination with blocking of STAT3 signaling improved immune cell trafficking and activation, thereby enhancing the efficacy of this combinatorial therapy in high-disease burden. Further, newly developed low-dose TMI shows enhanced immune modulation over conventional TBI, suggesting the benefits of localized targeted RT in hematological malignancies.
Hui:Janssen Research & Development, LLC: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal