


Introduction: The introduction of next-generation sequencing (NGS) has expedited the discovery of novel genetic lesions in acute myeloid leukemia (AML), thereby allowing better risk stratification with respect to overall survival (OS). We have previously reported that AML patients with PTPN11 and NPM1 mutations had longer OS following chemotherapy, while those carrying mutations in ASXL1, JAK2, RUNX1, TP53 and SRSF2 had a shorter OS (Daher-Reyes,ASH 2018). Little is known, however, regarding the impact of genetic profiles (somatic mutations and cytogenetic abnormalities) at initial AML diagnosis on the treatment outcomes following allogeneic hematopoietic stem cell transplantation (HCT).
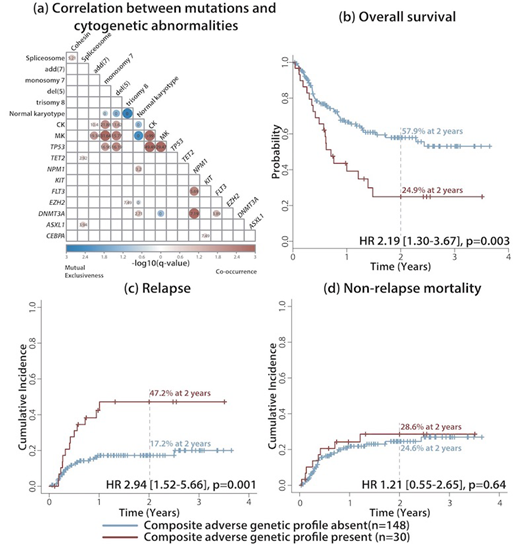
Methods & Patients: We enrolled AML patients who had available NGS data at time of initial diagnosis as part of the AGILE project between February 2015 and December 2018, and who subsequently underwent allogeneic HCT. NGS was performed on DNA samples isolated from peripheral blood or bone marrow samples at diagnosis. Analysis was performed using the TruSight Myeloid Sequencing Panel on the MiSeq sequencer (Illumina; San Diego, CA). Transplant outcomes (overall survival (OS), relapse-free survival (RFS), relapse incidence (RI), and non-relapse mortality (NRM)) after HCT were compared according to genetic profiles defined at diagnosis. Survival analysis for OS and RFS was performed using Cox's proportional hazard model, while the Fine-Gray model was used for RI and NRM analyses. Variables considered in the model included CR status prior to HCT (CR1 vs. beyond CR1), de novo AML (vs. secondary/therapy-related AML), induction chemotherapy used (3+7 vs. others), conditioning regimen (myeloablative vs. reduced intensity), WBC, age, donor type, mutation status of commonly mutated genes, and the composite adverse genetic profile (defined as having at least one of monosomal karyotype (MK), TP53 mutation, del(5), complex karyotype (CK), and monosomy 7), given that these 5 features were highly co-occurring, adverse prognostic factors (Figure 1A).
Results: We identified 435 patients in whom frontline NGS was performed, of whom a total of 178 patients (40.9%) received HCT and were included in the final analysis. A total of 598 (median 4, IQR 2-5) mutations were identified in 165 patients (n=165/178, 92.7%). Among 54 genes in the panel, 12 genes were mutated in more than 10% of the cohort, with the most commonly mutated genes being DNMT3A (30.3%), TET2 (25.3%), NPM1 (22.5%), RUNX1 (18.5%), IDH2 (16.9%), FLT3 (15.7%), ASXL1 (12.4%), BCOR (12.4%), CEBPA (11.2%), NRAS (11.2%), IDH1 (10.1%), and SRSF2 (10.1%).
In univariate analysis, the groups with a composite adverse genetic profile (n=30/178, 16.9%) showed decreased OS (HR 2.19 [1.30-3.67]; p=0.003), while patients harbouring spliceosome gene (SF3B1, SRSF2, U2AF1, and ZRSR2) mutations (n=37/178, 20.8%) had longer OS (HR 0.39 [0.18-0.85]; p=0.018), with 2-year OS rates of 24.9% and 57.9%, respectively (p=0.002)) (Figure 1B). The composite adverse genetic profile was also associated with shorter RFS (HR 2.23 [1.34-3.69]; p=0.002), while spliceosome gene mutations were associated with longer RFS (HR 0.42 [0.20-0.88]; p=0.022), with 2-year RFS rates of 23.7% vs. 57.9%, respectively (p=0.001)). The composite adverse genetic profile was also associated with higher RI (HR 2.94 [1.52-5.66]; p=0.001), with 2-year RI rates of 47.2% vs. 17.2%, respectively, for patients with and without adverse genetic features (p=0.002) (Figure 1C). Neither the composite adverse genetic profile, nor spliceosome gene mutations, were associated with NRM, with HR of 1.21 [0.55-2.65], p=0.64) and 0.45 [0.16-1.31], p=0.15, respectively (Figure 1D). Multivariate analyses confirmed that the composite adverse genetic profile and spliceosome gene mutations were independent prognostic factors for OS, RFS, and RI (p=0.004, p=0.002, and p=0.001, respectively) and for OS and RFS (p=0.020 and p=0.022, respectively).
Conclusion: In our cohort, the composite adverse genetic profile (i.e. having at least one of MK, TP53 mutation, del(5), CK and monosomy 7 remained as a poor prognostic factor even after allogeneic HCT. To clarify the role of genetic risk stratification in HCT, further analysis using a larger cohort is warranted. In addition, a comparative analysis between HCT vs no-HCT groups according to the genetic profile, is ongoing in a in a larger patient cohort.
Michelis:CSL Behring: Other: Financial Support. Mattsson:Gilead: Honoraria; Celgene: Honoraria; Therakos: Honoraria. Schimmer:Novartis Pharmaceuticals: Consultancy; Otsuka Pharmaceuticals: Consultancy; Jazz Pharmaceuticals: Consultancy; Medivir Pharmaceuticals: Research Funding. McNamara:Novartis Pharmaceutical Canada Inc.: Consultancy. Maze:Pfizer Inc: Consultancy; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees. Gupta:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Sierra Oncology: Honoraria, Membership on an entity's Board of Directors or advisory committees; Incyte: Honoraria, Research Funding; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. Yee:Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Astex: Research Funding; Hoffman La Roche: Research Funding; MedImmune: Research Funding; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Merck: Research Funding; Millennium: Research Funding; Astellas: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees. Minden:Trillium Therapetuics: Other: licensing agreement. Schuh:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Agios: Honoraria; Teva Canada Innovation: Honoraria, Membership on an entity's Board of Directors or advisory committees; Astellas: Honoraria, Membership on an entity's Board of Directors or advisory committees; Jazz: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal