

Introduction: Patients with lower-risk (LR) MDS, defined as very low-, low-, and intermediate-risk by the Revised International Prognostic Scoring System (IPSS-R), have a reduced risk of progressing to acute myeloid leukemia compared with higher-risk patients, but a shortened overall survival (OS) compared with age-matched controls. MDS patients with RS have a better prognosis than those without RS, but may experience extended periods of RBC transfusion dependence. RBC transfusion dependence is associated with reduced OS in patients with LR-MDS, but studies focusing on RBC transfusion dependence and OS in RS+ MDS patients are lacking. To address this gap, data from the Canadian MDS Registry were used to assess the relationship between RBC transfusion dependence patterns and OS in this patient population.
Methods: Patients with a diagnosis of RS+ MDS who were identified as transfusion dependent (TD) in the Canadian MDS Registry from 2008 to 2019 were included. Patients were considered TD if they received ≥ 1 RBC transfusion in at least one 8-week cycle. A sensitivity analysis was conducted wherein patients were considered TD if they received ≥ 1 RBC transfusion for 2 consecutive 8-week cycles. Patients were considered persistently TD (PTD) if they were TD throughout follow-up, or intermittently TD (ITD) if they were transfusion independent for periods of ≥ 8 weeks after an initial onset of TD. Covariates that were assessed included age, sex, IPSS-R risk score at enrollment, Eastern Cooperative Oncology Group performance status score at enrollment, ferritin level at first TD onset, Charlson Comorbidity Index at first TD onset, and receipt of iron chelation and anemia-treating therapies at first TD onset. Cox proportional hazards regression was used to test the association between PTD and mortality risk. Treatment patterns during follow-up were also examined.
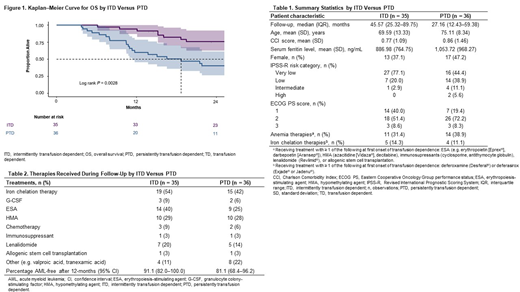
Results: Between 2008 and 2019, 191 patients had a diagnosis of RS+ MDS, of which 107 required ≥ 1 RBC transfusion over at least one 8-week cycle during follow-up. Of the 107 patients who received ≥ 1 RBC transfusion, 71 had ≥ 2 assessments for transfusion dependence and complete data on all outcomes and covariates, 36 (50.7%) of whom were classified as PTD (Table 1). Compared with ITD patients, PTD patients were older (mean age ± standard deviation [SD]: 75.11 ± 8.34 vs 69.59 ± 13.33 years) and had higher IPSS-R risk (17% of PTD patients were intermediate- or higher-risk compared with 3% of ITD patients). Median OS from first TD onset was 18.7 months (95% confidence interval [CI] 11.3-46.9) for PTD patients, compared with 48.7 months (95% CI 39.0-not evaluable) for ITD patients (Figure). After adjusting for baseline covariates, being PTD was associated with significantly greater mortality risk than being ITD (hazard ratio [HR] 2.24, 95% CI 1.18-4.25). Similar results were observed for the sensitivity analysis requiring ≥ 1 RBC transfusion for 2 consecutive 8-week cycles prior to the onset of TD (HR 2.18, 95% CI 1.13-4.21). Compared with ITD patients, PTD patients were less likely to receive iron chelation therapies (42% vs 54%), erythropoiesis-stimulating agents (25% vs 40%), and lenalidomide (14% vs 20%) during follow-up (Table 2).
Conclusions: In this study, we extracted Canadian MDS Registry data on RBC transfusions and OS for MDS patients with RS+ MDS. More than half (50.7%) of the identified cohort became TD during follow-up. Among those who received RBC transfusions, PTD patients had significantly shorter OS and increased mortality risk compared with ITD patients, and RBC transfusion dependence independently predicted inferior outcomes. These conclusions are consistent with previous findings on the relationship between RBC transfusions and OS in all patients with LR-MDS.
Buckstein:Takeda: Research Funding; Celgene: Consultancy, Honoraria, Research Funding. Keating:Celgene: Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria; Seattle Genetics: Consultancy; Janssen: Membership on an entity's Board of Directors or advisory committees; Shire: Membership on an entity's Board of Directors or advisory committees; Hoffman La Roche: Membership on an entity's Board of Directors or advisory committees; Sanofi: Membership on an entity's Board of Directors or advisory committees. Leber:Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Pfizer: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene Corporation: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Astellas: Honoraria, Membership on an entity's Board of Directors or advisory committees; Jazz: Honoraria, Membership on an entity's Board of Directors or advisory committees; Alexion: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Sabloff:Pfizer Canada:: Honoraria, Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Honoraria, Membership on an entity's Board of Directors or advisory committees; Sanofi Canada: Research Funding; Novartis Pharmaceuticals: Honoraria, Membership on an entity's Board of Directors or advisory committees; ASTX: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Astellas Pharma Canada: Honoraria, Membership on an entity's Board of Directors or advisory committees; Actinium Pharmaceuticals, Inc: Membership on an entity's Board of Directors or advisory committees. Leitch:Novartis: Honoraria, Research Funding, Speakers Bureau; Otsuka: Honoraria; Alexion: Research Funding; AbbVie: Research Funding; Celgene Corporation: Honoraria, Research Funding. St. Hilaire:Celgene: Honoraria, Research Funding; Novartis: Honoraria, Research Funding. Finn:Takeda: Membership on an entity's Board of Directors or advisory committees; Sanofi: Membership on an entity's Board of Directors or advisory committees; Ipsen: Membership on an entity's Board of Directors or advisory committees; Lundbeck: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Boehringer Ingelheim: Research Funding; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Merck: Research Funding; Alexion: Membership on an entity's Board of Directors or advisory committees; Astra Zeneca: Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria; Bristol Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees. Yee:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Astex: Research Funding; Hoffman La Roche: Research Funding; MedImmune: Research Funding; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Merck: Research Funding; Millennium: Research Funding; Astellas: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees. Banerji:Janssen: Consultancy, Honoraria, Research Funding; Research Manitoba: Research Funding; CAPhO: Honoraria; BIOGEN: Other: Licensing fee; CancerCare Manitoba/University of Manitoba: Employment; CIHR: Research Funding; Dana-Farber Cancer Institute: Other: Licencing fee; CCMF: Research Funding; Abbvie: Consultancy, Honoraria; Gilead: Consultancy, Honoraria, Research Funding; Astra-Zeneca: Consultancy, Honoraria; LLSC: Research Funding; Roche: Honoraria, Licensing fee, Research Funding. Liu:Celgene Corporation: Employment. Tang:Celgene Corporation: Employment, Equity Ownership. Westcott:Celgene Corporation: Employment, Equity Ownership. Huang:Celgene Corporation: Employment. Wang:Cornerstone Research Group: Employment. Cameron:Cornerstone Research Group: Employment, Equity Ownership. Morison:Celgene Corporation: Employment. Spin:Cornerstone Research Group: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal