

Background: In myelodysplastic syndromes (MDS), thrombocytopenia is associated with mortality and treatments in this setting are scarce. We tested whether eltrombopag, a thrombopoietin receptor agonist, be effective in improving outcomes in lower-risk MDS with severe thrombocytopenia within a multicentre clinical trial (EQoL-MDS). Initial interim results of short-term efficacy and safety have been published (Oliva et al. Lancet Hem 2017) in the first 90 subjects. We present interim results of the second phase for long-term results in the initial 90 of 174 subjects.
Methods: In a single-blind, randomised, controlled, phase 2 trial of adult patients with International Prognostic Scoring System (IPSS) low- or intermediate-1-risk MDS and severe thrombocytopenia. Adult patients with a stable platelet (PLT) count <30 Gi/L are randomized (2:1) to receive eltrombopag (50 mg to 300 mg) or placebo for at least 24 weeks and until disease progression. We report results of the second phase of the trial with primary endpoints duration of PLT response and long-term safety and tolerability. Amongst secondary endpoints, we present changes in quality of life (QoL), overall survival (OS) and leukemia-free survival (LFS).
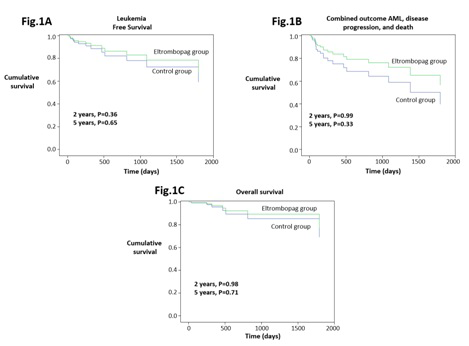
Results: The first 90 subjects were enrolled between 2011 and 2016. Characteristics of patients have been previously published (Lancet Hem 2017). PLT responses occurred in 28 (47.5%) of 59 patients in the eltrombopag group versus 1 (3.2%) of 31 patients in the placebo group (odds ratio 27.1 [95% CI 3.5-211.9], p=0.002) in median time 14 days (95% CI 7-40 days). Severe bleeding (WHO bleeding score ≥2) occurred in 19 patients, with a significantly higher incidence in the placebo (11 [35.3%] of 31 patients) than in the eltrombopag arm (8 [13.6%] of 59 patients; p=0.015). Sixty-eight grade 3-4 adverse events occurred in 30 of 59 (50.8%) eltrombopag patients versus 10 events in 6 of 31 placebo cases (19.4%;χ2=8,4, p=0.004, stopping rule not reached). The outcomes acute myeloid leukemia (AML) evolution, progression and death occurred in 5 (8.5%), 4 (6.8%), and 5 (8.5%), respectively of 59 eltrombopag cases versus 2 (6.5%), 3 (9.7%), 2 (6.5%), respectively of 31 placebo cases (P ranging from 0.69 to 1.00). Median LFS, combined outcome (AML, disease progression and death) and OS were not reached in the whole group. Differences in LFS, combined outcome and OS at 2 and 5 years by study arms were adjusted for baseline bone marrow blasts since the proportion of patients with >2% blasts (i.e. the median value of the whole study cohort) tended to be higher (P=0.06) in Eltrombopag (59.3%) than in placebo treated (38.7%) patients and resulted to be a strong predictor of study outcomes at both 2 and 5 years (P<0.002). The between-arm difference in LFS, combined outcome and OS at 2 and 5 years ranged from 0.33 to 0.99 (Fig.1 A-C). QOL-E and EORTC QLQ-C30 scores at baseline have been previously reported (Lancet Hem 2017). Within-arm longitudinal analyses showed that subjects on placebo experienced a significant worsening in QOL-E sexual domain (P=0.025) whereas subjects in the eltrombopag arm had a significant improvement in QOL-E MDS specific (P<0.001) and total scales (P=0.047) and a trend of improvement in QOL-E physical and social scores (both P=0.054). Between-arm comparison revealed that longitudinal changes in QOL-E MDS specific domain significantly differed between the two study arms in favour of eltrombopag (P=0.005). Finally, QOL-E functional (P=0.026), social (P<0.001), fatigue (P=0.01), MDS specific (P<0.001), general (P=0.001), treatment outcome index (P<0.001) and total scale (P<0.001) significantly improved with increasing PLT counts.
Conclusion. Eltrombopag is well-tolerated in patients with lower-risk MDS and severe thrombocytopenia and is clinically effective in raising PLT count and reducing bleeding events. QoL improves with response to treatment. The assessment of long-term safety and efficacy of eltrombopag and its effect on survival (phase 2 part of study) is still ongoing.
Oliva:Novartis: Consultancy, Speakers Bureau; Apellis: Consultancy; Celgene Corporation: Consultancy, Honoraria, Speakers Bureau. Alati:Pfizer: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Santini:Celgene Corporation: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Johnson & Johnson: Honoraria; Acceleron: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Menarini: Membership on an entity's Board of Directors or advisory committees. Giai:Pfizer: Honoraria; BMS: Honoraria; Novartis: Honoraria. Balleari:Celgene: Membership on an entity's Board of Directors or advisory committees. Ferrero:Novartis: Honoraria. Germing:Novartis: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Jazz Pharmaceuticals: Honoraria; Amgen: Honoraria. Fenaux:Aprea: Research Funding; Jazz: Honoraria, Research Funding; Celgene Corporation: Honoraria, Research Funding; Astex: Honoraria, Research Funding. Palumbo:Amgen: Honoraria; Celgene: Honoraria; Janssen: Honoraria; Novartis: Honoraria; Teva: Honoraria; Hospira: Honoraria. Liberati:Novartis: Other: Clinical trial support; Janssen: Honoraria; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Clinical trial support; Roche: Other: Clinical trial support; Amgen: Membership on an entity's Board of Directors or advisory committees, Other: Clinical trial support; Celgene: Honoraria, Other: Clinical trial support; Bristol-Myers Squibb: Honoraria; Takeda: Membership on an entity's Board of Directors or advisory committees; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees; Incyte: Consultancy. Molteni:Celgene: Membership on an entity's Board of Directors or advisory committees. Buccisano:Astellas: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Bocchia:Novartis: Honoraria; Incyte: Honoraria; BMS: Honoraria. Candoni:Merck SD: Honoraria, Speakers Bureau; Gilead: Honoraria, Speakers Bureau; Celgene: Honoraria; Pfizer: Honoraria; Janssen: Honoraria. Martino:Bristol myers squibb: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees. Latagliata:Janssen: Honoraria; Novartis: Honoraria; Pfizer: Honoraria; Celgene: Honoraria.
Eltrombopag is indicated for: 1. the treatment of patients aged 1 year and above with primary immunethrombocytopenia (ITP) lasting 6 months or longer from diagnosis and who are refractory to other treatments; 2. in adult patients with chronic hepatitis C virus (HCV) infection for the treatment of thrombocytopenia, where the degree of thrombocytopenia is the main factor preventing the initiation or limiting the ability to maintain optimal interferon-based therapy; 3. in adult patients with acquired severe aplastic anaemia who were either refractory to prior immunosuppressive therapy or heavily pretreated and are unsuitable for hematopoietic stem cell transplantation

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal