

Introduction: Diffuse large B-cell lymphoma (DLBCL), is a genetically and clinically heterogeneous disease. Building on existing clinical prognostic scores in the era of genomic risk modeling is critical to improve patient (pt) outcomes and inform future trials. With advances in next-generation sequencing, the interrogation of genetic drivers to refine prognostic subgroups over and above histological cell of origin (COO) subtypes has been of keen interest. The application of an unsupervised prognostic clustering approach, non-negative matrix factorization (NMF) algorithm, to whole exome sequence (WES) data has led to identification of six distinct molecular clusters with potential clinical relevance (Chapuy et al. Nature Med, 2018). Here, we applied the NMF clustering approach to targeted exome-sequencing data utilizing the FoundationOne HemeTM panel and analyzed RNA gene expression data from the randomized Phase 3 GOYA and Phase 1b/2 CAVALLI studies in de novo DLBCL.
Methods: Biopsy samples, clinical outcomes (overall survival [OS], progression-free survival [PFS]), and targeted exome-sequencing data were available for 499 pts from the GOYA trial (NCT01287741; ITT=1418; obinutuzumab [G]-CHOP vs rituximab [R]-CHOP) and 106 pts from the CAVALLI trial (NCT02055820; ITT=267, venetoclax+[G/R]-CHOP). The FoundationOne HemeTM panel of 465 genes (F1H, Foundation Medicine Inc. [FMI]) was used to define single nucleotide variants, copy number amplifications, and rearrangements. Clustering methodology was implemented using the R package NMF (Gaujoux and Seoighe, BMC Bioinformatics 2010). All models were adjusted for treatment (where applicable), age, International Prognostic Index (IPI), sex, COO (NanoString), and BCL2 by IHC.
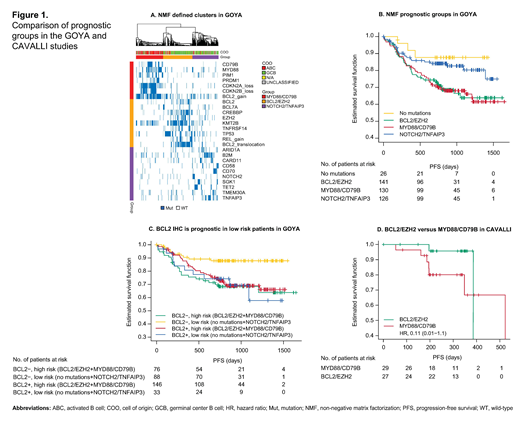
Results: Applying the NMF algorithm, de novo pts in GOYA clustered similarly into four of the six groups recently reported by Chapuy et al.: MYD88/CD79B, BCL2/EZH2, NOTCH2/TNFAIP3, and no mutations (Fig 1A). The mutation profiles and COO subset distribution were also similar to those previously described. Furthermore, the MYD88/CD79B and BCL2/EZH2 groups remained associated with inferior clinical outcomes (Fig 1B), with observed poor prognosis over the NOTCH2/TNFAIP3 and no mutations groups (OS: hazard ratio [HR], 2.0; 95% CI: 0.97, 3.90; PFS: HR, 1.60; 95% CI: 0.93, 2.80), even when adjusting for known prognostic factors. Application of NMF to pts treated with the BCL2-inhibitor venetoclax in combination with R-CHOP (CAVALLI) yielded only MYD88/CD79B- and BCL2/EZH2-like groups due to enrollment. However, in contrast to the BCL2/EZH2 subgroup reported in both Chapuy et al. and GOYA, these pts demonstrated a trend towards improved outcomes over MYD88/CD79B (OS: HR, 0.12; 95% CI: 0.01, 1.60; PFS: HR, 0.11; 95% CI: 0.01, 1.10; Fig 1D). The difference between studies is potentially explained by the ability of venetoclax treatment to overcome the adverse prognostic impact of BCL2 over-expression. BCL2 IHC positive (BCL2+) pts were enriched in high-risk groups in GOYA (MYD88/CD79B and BCL2/EZH2) (odds ratio [OR], 5.0; 95% CI: 3.13, 8.33) and CAVALLI (MYD88/CD79B) (OR, 2.0; 95% CI: 0.63, 6.67). In GOYA, a prognostic trend for BCL2+ status is observed within low-risk pts (OS BCL2+ HR, 1.9; 95% CI: 0.55, 6.3; PFS BCL2+ HR, 2.7; 95% CI: 1.0, 6.8), but not within high-risk groups (OS BCL2+ HR, 0.55; 95% CI: 0.29, 1.00; PFS BCL2+ HR, 0.76; 95% CI: 0.45, 1.30; Fig 1C). Additional genetic risk models will be presented, e.g. as per Reddy et al. (Cell, 2017), as well as differential expression analysis.
Conclusions: Important findings from the present work include: 1) utility of targeted mutational data from F1H in recapitulating molecular clusters, previously identified using WES, that further subclassify established prognostic groups such as COO and IPI; and 2) a trend towards improved survival outcomes for patients in the BCL2/EZH2 cluster upon treatment with the BCL2 inhibitor venetoclax. This highlights the potential for utilizing novel genetic signatures as a means of identifying patients suitable for targeted therapies in the era of personalized health care.
Kim:Genentech, Inc.: Employment. Fan:Genentech, Inc.: Employment. Bolen:F. Hoffmann-La Roche: Equity Ownership; Genentech, Inc.: Employment. Bazeos:Roche Products Ltd: Employment, Equity Ownership. Jiang:Genentech: Employment, Equity Ownership; F. Hoffman-La Roche: Equity Ownership. Balasubramanian:Roche-Genentech: Employment; F. Hoffman-La Roche: Equity Ownership. Balakrishnan:Genentech, Inc.: Employment. Knapp:F. Hoffmann-La Roche Ltd: Employment. Humphrey:F. Hoffmann-La Roche Ltd: Employment. Nielsen:F. Hoffmann-La Roche Ltd: Employment, Equity Ownership. Venstrom:F. Hoffmann-La Roche Ltd: Employment. Hernandez:Genentech, Inc.: Employment, Equity Ownership. Paulson:F. Hoffman-La Roche: Equity Ownership; Genentech: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal