

ABSTRACT:
INTRODUCTION: ELN-2017 guideline is the gold standard for risk stratifying AML patients. However, clinical prognostic factors such as age are not incorporated into the guideline. Therefore, we examined if novel prognostic models incorporating clinical factors and expression of select transcripts can improve the current guideline. The prognostic models were developed utilizing molecular data from unsorted mononuclear cells (MNCs) and viable leukemic blasts (VLBs).
METHODS: Specimens were obtained from untreated AML patients (N=383) who received intensive chemotherapy on SWOG trials S9031, S9333, S0106 and S0112. Patients were randomly separated into discovery (N=190) and validation (N=193) cohorts. Participants provided informed consent in compliance with the Declaration of Helsinki, SWOG, NCI, and Fred Hutch regulations. VLBs were isolated using fluorescence-activated cell sorting (FACS, Pogosova et al., 2018, Biopreserv Biobank 16;42-52). RNA and DNA were extracted from MNCs and VLBs. FLT3-ITD, NPM1, CEBPA, ASXL1, RUNX1 and TP53 mutations were identified using fragment analyses and NGS. Transcript expression for BAALC, CEBPA, CCNA1, CD34, ERG1, EVI1, FLT3, GATA2, IL3RA, JAG1, KIT, MN1, RUNX1, and WT1 was quantified using Q-RT/PCR assays. Specimen attributes across paired samples were compared using McNemar's test and the Wilcoxon signed rank test. Associations with overall survival (OS), relapse-free survival (RFS), and complete remission (CR) were assessed using the Kaplan-Meier method, Cox proportional hazards regression, and logistic regression. Models were built in the discovery cohort using a pre-defined 3-step process of variable selection and 5-fold cross validation of this process; final model performance was evaluated in the validation cohort.
RESULTS:
Mutations, transcripts and clinical variables. Mutation frequencies, FLT3-ITD AR, and clinical outcomes were not significantly different between discovery and validation cohorts. The percentage of patients with high FLT3-ITD AR (per ELN-2017 definition) was increased in the VLBs compared to MNCs (77% vs 66%, respectively); FLT3-ITD AR was reclassified for 19 patients. Transcript expression was significantly increased in VLBs relative to MNCs for 8 transcripts (P<.02), while none of the transcripts was expressed at significantly lower levels in VLBs. Increasing FLT3-ITD AR in MNCs, but not VLBs, was associated with worse OS. Increased expression of CCNA1, ERG1, EVI1, FLT3, IL3RA, KIT and MN1 was significantly associated with adverse risk for one or more clinical outcome in MNCs and/or VLBs (P<.05). Increasing age, adverse cytogenetics, poor performance status (PS), secondary AML status, and adverse ELN risk group were significantly associated with inferior clinical outcomes in both MNCs and VLBs (P<.05).
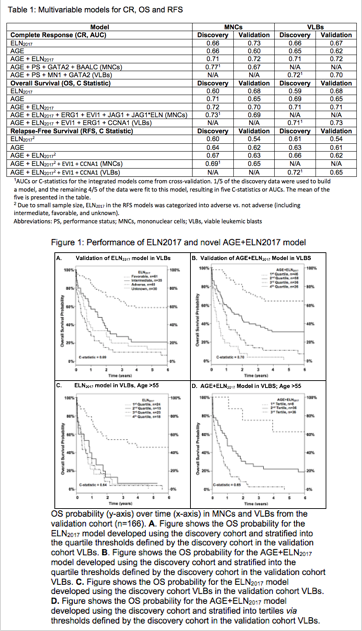
Model Development and Performance. Multivariable models for CR, OS, and RFS were fit using age, ELN-2017 risk group, PS, AML onset, immunophenotype, clinical trial, and combinations of these baseline variables as covariates. In the discovery cohort, the models with the best performance were obtained when clinical variables and transcript expression were integrated; however, these integrated models were not superior to AGE+ELN2017 models in the validation cohort (Table 1), whether utilizing molecular data from MNCs or VLBs. Quartile risk groups from the AGE+ELN2017 model displayed increased discrimination with respect to OS than the ELN risk groups (Figure 1A,B). The discriminative performances of the ELN2017 and AGE+ELN2017 models for OS were also examined in older adults (age ≥55). Given the small numbers of patients, risk scores for the AGE+ELN2017 model were divided into tertiles to identify 3 risk groups. The three risk groups derived from the AGE+ELN2017 scores showed increased ability to discriminate for projected OS relative to ELN2017 risk groups (Figure 1C, D).
DISCUSSION: ELN2017 models were significantly associated with clinical outcomes, but AGE+ELN2017 models may perform slightly better than ELN2017 models. Models incorporating selected transcript expression did not improve the ELN2017 models, whether transcripts were examined in MNCs or VLBs. While ELN-2017 prognostic guideline remains a critical tool for risk stratifying AML patients, the findings highlight the need for additional prognostic factors, including age, to improve the accuracy of risk stratification.
Othus:Celgene: Other: Data Safety and Monitoring Committee; Glycomimetics: Other: Data Safety and Monitoring Committee. Erba:Agios, Amgen, Astellas Pharma, Daiichi Sankyo, ImmunoGen, Janssen, Jazz Pharmaceuticals, Juno, Millennium, Seattle Genetics: Research Funding; Celgene, Incyte, Novartis: Speakers Bureau; Amgen, Celgene, Daiichi Sankyo, ImmunoGen, Incyte, Jazz Pharmaceuticals, Millennium, Novartis, Ono, Pfizer, Seattle Genetics, Sunesis: Consultancy. List:Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding. Radich:Novartis: Other: RNA Sequencing; TwinStrand Biosciences: Research Funding. Willman:to come: Patents & Royalties; to come: Membership on an entity's Board of Directors or advisory committees; to come: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal