

Introduction:Acute Myeloid Leukemia (AML) predominantly affects the older population, with a median age at diagnosis of 67 years (yrs). In the last decades, Overall Survival (OS) has not changed meaningfully for these patients (pts). This worse outcome is explained by the poor-risk biological profile of the disease but also by the scarce propensity in administering curative treatments in this age category. Despite this general attitude, there is consensus that age alone should not be representative of the functional profile of older pts and that making decisions based on the sole age parameter can compromise possible therapeutic attempts. Therefore, a panel of experts from SIE (Italian Society of Hematology),SIES (Italian Society of Experimental Hematology) and GITMO (Italian Group for Bone Marrow Transplantation) summarized a list of operational criteria to be used in the process of treatment allocation, identifying 3 fitness categories of patients to address to differentiated strategies: 1)Fit pts (FP), eligible to intensive chemotherapy (IC) with the aim to achieve complete remission (CR); 2)Unfit pts (UP), eligible to non-intensive chemotherapy (NIC) with the aim to prolong survival; 3)Frail pts (FP) for whom, since the natural course of disease cannot be altered, supportive therapy (ST) is the best option in the attempt to preserve an acceptable quality of life (Ferrara et. al, Leukemia 2013).
Aim: We retrospectively applied the operational SIE, SIES, GITMO criteria to a series of 180 consecutive non-APL AML pts diagnosed at our institution from 2013 to 2018 to investigate (1) the degree of concordance between the "operational criteria derived categories" and the actual treatment received; (2) the impact of this evaluation on long-term OS.
Methods: We analyzed 180 consecutive pts with AML (median age 66 yrs, range 21-91) diagnosed at our institution from January 2013 to December 2018. We mainly focused on 125 pts older than 60 yrs (median 70 yrs, range 61-91). For the purpose of comparison, 55 younger pts, submitted to IC (51/55, 93%), were also analyzed.
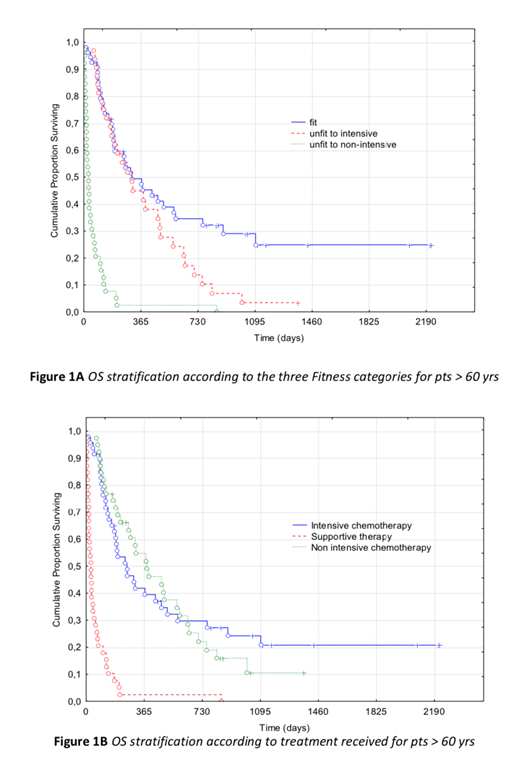
Results: SIE, SIES, GITMO operational criteria were retrospectively applied through medical files backtracking. One-hundred-48 out of 181 pts were stratified according to ELN 2010 as follow: 24 (16%) low risk, 59 (40%) intermediate-I, 25 (17%) intermediate-II and 40 (27%) high risk. This risk stratification did not differ between younger and older pts, suggesting that risk distribution may not be always an age-related factor. Overall, according to physician choice, 98 pts were submitted to IC, 40 to NIC, 42 to ST (54%, 22%, 24%, respectively). When focusing on pts older than 60 yrs, 47/125 were submitted to IC, 39/125 to NIC, 39/125 to ST (38% vs. 31% vs. 31%, respectively). A high concordance between treatment actually given and the one derived from the application of the "operational criteria" (165/180, 92%) was observed. The highest concordance was observed for the association of ST with FrP (39/40, 98%), whereas the associations IC with FP (96/107, 90%) and NIC with UP (30/33, 91%) showed a lower level of concordance. Overall, by applying the "operational criteria" the 3 categories differed significantly in terms of OS: 15,3 mos (range 0,4-78) for FP, 8,6 mos (range 2,2-47,9) for UP and 1 mos (range 0,1-29,9) for FrP, respectively (p<0.001). For pts older than 60 yrs, OS was 9,1 mos (range 0,4-78), 9,2 mos (range 2,2-47,9) and 1 mos (range 0,1-29,9) for FP, UP and FrP, respectively (p<0.001) (Fig. 1A). According to the treatment actually received, OS of pts older than 60 yrs was 6,9 mos (range 0,4-78) for IC, 11.0 mos (range 2,2-47,9) for NIC and 1 mos (range 0,1-29,9) for ST, respectively (p<0.001) (Fig. 1B).
Conclusions: In our real-life analysis, we confirmed that SIE, SIES, GITMO "operational criteria" represent a powerful tool to discriminate categories of older pts with different outcome.In pts older than 60 years, it was observed a high degree of concordance (>90%) between the "operational criteria" and the actual treatment delivered. However, long-term OS was longer when plotted according to the 3 fitness categories rather than to treatment intensity stratification (Fig.1 A and B). Such a discrepancy can be explained by a higher incidence of toxicity/early mortality in the IC group and also by a suboptimal application of treatment selection criteria. Reproducibility of operational criteria applications in a prospective fashion is currently underway.
Venditti:Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees; Daiichi-Sankyo: Consultancy, Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees; Abbvie: Consultancy. Buccisano:Janssen: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal