

The increased incidence of chronic lymphocytic leukemia (CLL) in first-degree relatives of affected patients indicates an element of genetic susceptibility to this malignancy, borne out in large scale genome-wide association studies (GWAS), which have identified over 40 constitutional risk alleles. Given the important genetic contribution to CLL susceptibility we hypothesized that constitutional genetic variants also affect disease progression. We employed GWAS methods in a large United Kingdom multi-center cohort study of well-characterized predominantly early-stage CLL cases to identify risk alleles for progressive CLL.
We conducted six GWAS for single nucleotide polymorphisms (SNPs) associating with progressive CLL incorporating a total of 774 cases of European ancestry recruited to 6 clinical centers across the United Kingdom. CLL cases were genotyped on the Illumina OmniExpress platform and genotypes were determined using Illumina GenomeStudio software. After imputation, we combined the association test statistic for 5,199,911 autosomal SNPs common to all 6 GWAS after exclusion of those with an imputation quality score of <0.9 and a minor allele frequency (MAF) of < 2.5%, and conducted a meta-analysis under a fixed-effect model. The primary outcome assessed was time to first treatment (TTFT), defined as the interval between CLL diagnosis and first treatment or last follow-up.
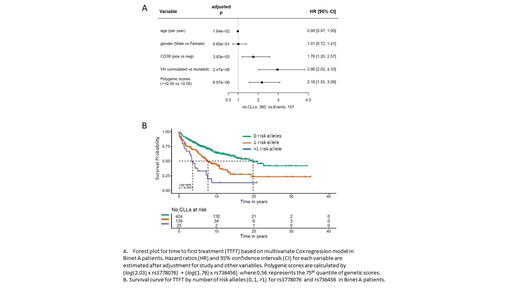
Pooling data from the 6 GWAS identified 5 SNPs at two genomic locations that surpassed genome-wide significance (P ≤ 5 x 10-8) for association with TTFT. The strongest statistical evidence for an association with progressive disease was for rs736456 (hazard ratio (HR) = 1.76, 95% confidence interval (CI) = 1.45-2.14; P = 1.26 x 10-8), which maps to chromosome 10q26.13. The second strongest association with progressive disease was for rs3778076 (HR = 2.03, 95% CI = 1.58-2.62; P = 3.89 x 10-8) which maps to chromosome 6p. Both markers showed consistent direction and magnitude of effect sizes across all six GWAS with no evidence of heterogeneity, and retained prognostic significance in multivariate models for disease progression, particularly in models restricted to Binet A patients. Whilst not as powerful as IGVH status, rs736456 and rs3778076 had prognostic utility equivalent to CD38 status, and are particularly powerful when considered together, identifying 5% of CLL patients carrying 2 or more risk alleles at high risk of progressive disease (Figure).
To identify cis-regulated genes at each locus associated with progressive disease we interrogated gene expression data derived from a meta-analysis of 31,624 blood samples collated by the eQTLGen consortium. Of the thirteen genes annotated to within 1Mb of the chromosome 10 association signal rs736456 is eQTL for the PLEKHA1 gene (TAPP-1)(Benjamini-Hochberg corrected P-value [PBH] = 1.29 x 10-15). Of the 27 genes annotated to within 1Mb of the chromosome 6 signal, rs3778076 is eQTL for 5 genes including UHRF1BP1 (PBH = 6.73 x 10-139) and C6ORF106 (PBH = 3.54 x 10-64). Annotated genes at both loci have been implicated in modulating B-cell receptor or innate immune responses, key pathways in CLL pathogenesis.
Data on post-treatment survival were available on 390 CLL cases, with 231 deaths and 159 censored at last follow-up, and neither the lead SNP at chromosome 10 or chromosome 6 were significantly associated with post-treatment survival in patients primarily treated with regimens that included chlorambucil, fludarabine or cyclophosphamide. It will be important to determine whether these markers predict overall survival in patients treated with novel targeted therapies.
Taken together, these data identify rs736456 and rs3778076 as prognostic in early stage CLL patients demonstrating that progression of CLL from asymptomatic to symptomatic disease is determined by constitutional genetic variation as well as the more established somatic drivers. Constitutional genetic markers have the advantage of being easy to perform, highly reproducible and inexpensive making them ideal for incorporation into multivariate prognostication models for early stage CLL.
Fegan:Roche: Honoraria; Janssen: Honoraria; Gilead: Honoraria; Abbvie: Consultancy, Other: Conference attendance sponsorship. Forconi:Gilead Sciences: Research Funding; Janssen-Cilag: Consultancy, Honoraria, Other: Travel, Accommodations, Expenses, Speakers Bureau; Novartis: Honoraria; Menarini: Consultancy; Abbvie: Consultancy, Honoraria, Other: Travel, Accommodations, Expenses, Speakers Bureau; Roche: Honoraria. Schuh:AbbVie: Consultancy, Speakers Bureau; Genentech: Consultancy, Speakers Bureau; Pharmacyclics: Consultancy, Speakers Bureau; Verastem: Speakers Bureau; Gilead: Speakers Bureau; Seattle Genetics: Speakers Bureau; Jazz Pharmaceuticals: Speakers Bureau; Bristol-Myers Squibb: Research Funding; Janssen: Speakers Bureau; Kite: Speakers Bureau. Hillmen:Pharmacyclics LLC, an AbbVie Company: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses, Research Funding; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses, Research Funding; Roche: Research Funding; Gilead: Research Funding; Apellis: Research Funding; Acerta: Membership on an entity's Board of Directors or advisory committees. Pratt:Binding Site, Amgen, Takeda, Janssen, Gilead: Consultancy, Honoraria, Other: Travel support.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal