

Survival rates of children with relapsed/refractory (r/r) BCP-ALL remain unsatisfactory and little progress has been made in the past 2 decades. Similarly, relapse of childhood B-NHL is usually associated with an aggressive disease and poor outcomes. Targeted immunotherapy with T-cells genetically modified to express a CD19-directed CAR showed an unprecedented antitumor efficacy, leading to the recent FDA and EMA approval of two CD19-CAR products for treatment of BCP-ALL and B-NHL. Relevant toxicities have, however, been reported, mainly related to the development of severe Cytokine Release Syndrome (CRS) and/or of neurotoxicity.
At Ospedale Pediatrico Bambino Gesù (OPBG) in Rome, we developed a clinical-grade, 2nd generation, CD19-specific CAR construct, including 4.1bb as costimulatory domain and the inducible caspase-9 safety switch (iC9-CD19-CAR), vehiculated by a retroviral vector, to conduct an academic, phase I/II clinical trial in patients (age 1-25 yrs) affected by BCP-ALL or B-NHL. We now report on the results of the phase I and of the first 8 patients treated in the phase II portion of the study, in terms of feasibility, toxicity, maximum tolerated/recommended dose (MTD/RD) and data on response rate and biological correlates.
The phase I, dose-escalation portion of the study included 3 dose levels (DL), namely: DL1, 0.5×106; DL2, 1.5×106; DL3, 3.0×106 CAR+ T cells per kg of recipient body weight. In the phase II portion, patients were treated at the RD identified in the phase I, namely 3.0×106 CAR+cells/kg. All patients received a lymphodepleting regimen consisting of fludarabine and cyclophosphamide for 3 days and iC9-CD19-CAR T cells were subsequently administered as single infusion. Patients were monitored for toxicity, expansion and persistence of iC9-CD19-CAR T cells.
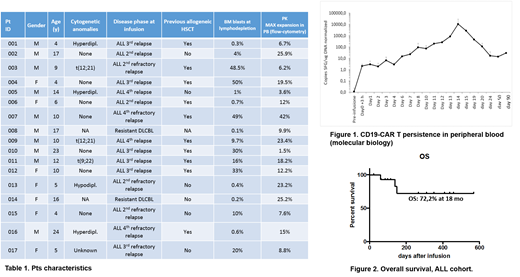
Seventeen children were enrolled into the trial and received iC9-CD19-CAR T cells between January 2018 and June 2019. Data were analyzed as of July 20, 2019. The characteristics of the patients are detailed in table 1. The designed dose concentration was successfully produced for all the enrolled patients and we did not observe any production failure. The median transduction rate in the drug product was 54% (range 21-73), while the median vector copy number was 3.8 (range 2.8-6.2). During the phase I portion of the study, no dose limiting toxicities (DLTs) have been recorded, defining the MTD as 3.0×106 CAR+ T cells per kg of recipient body weight. The treatment was overall tolerated and all the toxicities were reversible, the most severe being grade 3-4 neutropenia, thrombocytopenia and/or anemia, occurring in 16/17 (94.1%) patients; in 13/16 patients (81.2%) the hematological toxicity developed before the infusion and persisted after the administration of CAR T cells. Cytokine release syndrome (CRS) occurred in 10/17 patients (58.8%) and was overall moderate, reaching grade 3 (Lee criteria) in one patient only. Notably, none of the patients developed neurotoxicity and no activation of the safety switch was required. All patients were assessed for response at 4 weeks from iC9-CD19-CAR T cell infusion and 13/15 (86.7%) patients with ALL achieved complete remission (CR) with negativity of minimal residual disease (MRD), including 2/3 patients receiving the DL1, 9 patients who had failed a previous allogeneic haematopoietic stem-cell transplantation (HSCT) and 6 patients that had previously received blinatumomab, as CD19-directed immunotherapy. The iC9-CD19-CAR T cells expanded in vivo and were detectable by both flow-cytometry and molecular biology in the blood (Fig.1), bone marrow and cerebrospinal fluid of the responders. One CD19-negative relapse 3 months after infusion was recorded, while 3 additional patients relapsed with CD19+ leukemia blasts. Four patients received HSCT while in CR with MRD negativity because of regrowth of normal CD19+ B cells. The 18-month probability of overall survival for the BCP-ALL cohort is 72.2% (Fig.2). One of the 2 B-NHL patients showed a partial response.
Our data indicate that iC9-CD19-CAR T cell in an academic setting is feasible, safe and extremely effective in treating highly resistant/relapsed BCP-ALL. In our trial, no major or life-threatening toxicities were observed and, despite the moderate CRS recorded, high rates of CR were achieved, suggesting that the combination of a retroviral platform and 4.1bb as costimulation is able to mediate a potent antitumor effect
Merli:Amgen: Honoraria; Novartis: Honoraria; Sobi: Consultancy; Bellicum: Consultancy. Algeri:Bluebird bio: Consultancy, Honoraria; Atara Biotherapeutics: Consultancy, Honoraria; Miltenyi: Honoraria. Locatelli:Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Bellicum: Consultancy, Membership on an entity's Board of Directors or advisory committees; bluebird bio: Consultancy; Miltenyi: Honoraria; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal