

Background:
In general, modern clinical trials for pediatric acute lymphoblastic leukemia (ALL) have intensified therapy compared with therapy in prior decades. While survival rates now approach 90%, increased treatment intensity has heightened the risk of complications such as serious infections or organ toxicities, which may in turn lead to dose modifications and/or treatment delays. There is a paucity of data on the prognostic impact of cumulative delays during the intensive phases of ALL therapy.
Methods:
We performed a retrospective chart review of patients between the ages of 1-21 years with newly diagnosed ALL who were treated at two large academic pediatric hospitals that are part of the Leukemia Electronic Abstraction of Records Network (LEARN). Eligible patients were those diagnosed with B- or T-lineage ALL who received chemotherapy treatment at least through the start of maintenance therapy. Exclusion criteria included disease relapse prior to start of maintenance, Down syndrome, or clinical features requiring highly intensified frontline therapy. The primary study objective was to determine the impact of treatment delays on relapse-free survival (RFS) and overall survival (OS). A secondary objective was to investigate associations between delays and patient clinical characteristics.
Results:
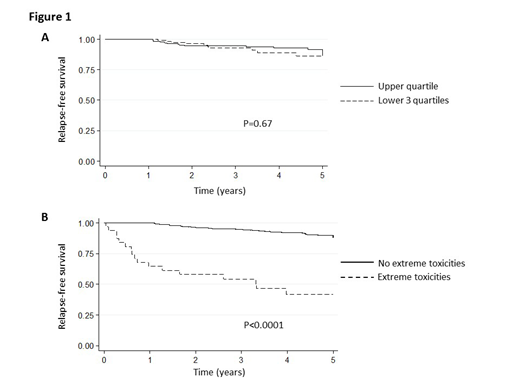
A total of 537 patients were eligible for analysis. Of these 537, 32 were analyzed separately as an "extreme toxicity" subgroup, due to excessive treatment-related morbidities prior to the start of maintenance requiring significant therapy modification. The remaining 505 were divided into quartiles based on their duration of delay, with the highest quartile experiencing >64 days of delay to start of maintenance. Most patients experienced some delay (median 40 days, range 0-154 days). Patients in the highest quartile were characterized by an older mean age at diagnosis (7.8 versus 6.7 years, p=0.0254), treatment on a more intensified regimen (p<0.001), and higher likelihood of Hispanic or Asian race/ethnicity (p=0.033). These patients did not have a significantly lower RFS (4.7 vs. 4.8 years; p=0.701; Figure 1A Kaplan-Meier [KM] p=0.67) or OS (4.8 vs. 4.9 years; p=0.24) compared to patients in the other three quartiles. Patients in the extreme toxicities group did demonstrate a significantly inferior RFS (2.9 vs. 4.7 years; p<0.001; Figure 1B KM p<0.0001)) and OS (3.2 vs. 4.9 years; p<0.001) compared with the remainder of patients. Patients in the extreme toxicities group were more likely to be Hispanic or black (p=0.039), have T-ALL (p=0.043), have received higher intensity therapy (p=0.005), and have a higher mean age at diagnosis (11.8 vs 7.0 years; p<0.0001).
Conclusions:
Due to the intensity of modern ALL therapy, treatment delays are common. Our data suggest that prolonged delays in treatment prior to the start of maintenance therapy do not impact survival, but that extreme toxicities requiring significant alterations in therapy are associated with significantly poorer RFS and OS.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal