

Introduction: Pregnancies in women with Sickle Cell Disease (SCD) are at risk of adverse maternal and fetal outcomes. There are no studies characterizing features predictive of pregnancy-related complications that would enable targeted interventions towards those at high-risk, whilst avoiding exposure of those at low risk to the potential intervention-associated complications.
Objective: To explore risk factors associated with adverse pregnancy outcomes in women with SCD and to develop a prediction rule identifying women at different levels of risk for adverse pregnancy outcomes.
Methods: Retrospective cohort study of pregnant women with SCD at a tertiary care center. Maternal composite outcome (MCO) includes any of the following: severe, complicated anemia, multi-organ failure, venous thromboembolism, vaso-occlusive episodes requiring admission, blood transfusion, maternal mortality, hypertensive disorder of pregnancy (HDP), cardiac, pulmonary, hepatobiliary, MSK/skin, splenic, neurologic, or renal complication. Fetal composite outcome (FCO) includes any of the following: perinatal mortality, preterm birth, or small for gestational age size. Both composite outcomes were defined a priori. SCD-associated MCO were defined based on a published classification of SCD manifestations. HDP were divided to include gestational hypertension or pre-eclampsia, as noted in the health record. For twin pregnancies, the FCO was considered present if either infant met criteria. Predictor variables included SCD-related and non-SCD related maternal factors, which have been shown in the literature and through clinical experience to potentially result in adverse pregnancy outcomes. For a variable to be interpreted as a potential cause of an adverse outcome, it must have been present before the outcome and must not have been part of the outcome definition. Regression models for MCO and FCO were constructed using generalized estimation equation (GEE) logistic regression with clustering by woman to account for non-independence of outcomes in women with several pregnancies during the study period. From a set of 21 potential predictors for MCO and 26 potential predictors for FCO, those with univariate p-values <0.2 in GEE were included in a multivariable GEE regression model. Using cross-validation, predictive performance of the fitted model was evaluated using the concordance statistic and accuracy of prediction using a calibration curve; for each of 10 90%:10% splits of the dataset, a model was fitted on the 90% and used to obtain predicted probabilities on the 10%.
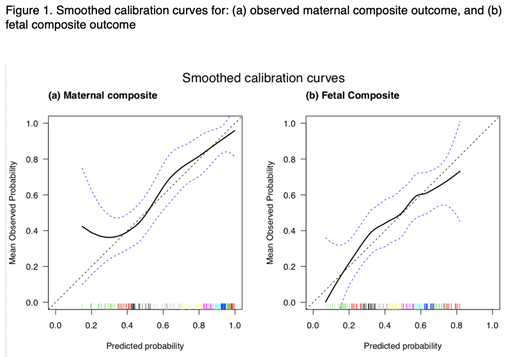
Results: Of 199 pregnancies in 131 women between 1990 and 2016, MCO and FCO occurred in 71% and 45% of pregnancies, respectively. Risk for MCO was predicted by low maternal BMI, low first-trimester hemoglobin, VOE in the year preceding pregnancy, high LDH in pregnancy, history of multiple transfusions, and history of cardiac complications (heart failure, cardiomyopathy, or cardiomegaly). While presence of MCO was not part of the model given the inability to include it in a prediction rule for primiparous women, its manifestation was a risk factor for recurrence in subsequent pregnancies. FCO risk was predicted by older maternal age, high LDH in pregnancy, and maternal composite outcome during pregnancy. The model was discriminative for (a) MCO with a concordance statistic of 0.84 (se=0.03) on the observed data, and a cross-validated value of 0.80 (se=0.03), and (b) FCO with a concordance statistic of 0.72 (se=0.04) on the observed data, and a cross-validated value of 0.69 (se=0.04). Except at the extremes, predicted risk agreed well with observed risk for both the MCO and the FCO (Figure 1). Predicted risk of the MCO, separated pregnancies into groups having as low as a 35% to as high as a 95% chance, while predicted risk of FCO separated pregnancies into groups as low as 10% to as high as 70% (Figure 1).
Conclusions: Our study shows that readily available clinical and laboratory variables can predict the degree of risk for an adverse pregnancy outcome in women with SCD. In our models, SCD genotype itself does not predict adverse maternal or fetal outcome, while presence of MCO or FCO are important predictors alongside other prespecified variables. The prediction rules will enable identification of sub-groups of women at higher risk of adverse events, allowing for consideration of targeted interventions such as prophylactic transfusion.
Malinowski:Alexion: Consultancy, Honoraria. Kuo:Agios: Consultancy; Alexion: Consultancy, Honoraria; Apellis: Consultancy; Bioverativ: Other: Data Safety Monitoring Board; Pfizer: Consultancy; Bluebird Bio: Consultancy; Celgene: Consultancy; Novartis: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal