

Key Points
In a real-life CLL cohort still on ibrutinib after 3 years, 57% of patients with residual clonal lymphocytosis had a BTK mutation.
The presence of a BTK mutation in patients still on ibrutinib conferred a greater likelihood of subsequent CLL progression.

Abstract
Mutational analyses performed following acquired ibrutinib resistance have suggested that chronic lymphocytic leukemia (CLL) progression on ibrutinib is linked to mutations in Bruton tyrosine kinase (BTK) and/or phospholipase Cγ2 (PLCG2) genes. Mutational information for patients still on ibrutinib is limited. We report a study aimed to provide a “snapshot” of the prevalence of mutations in a real-life CLL cohort still on ibrutinib after at least 3 years of treatment. Of 204 patients who initiated ibrutinib via an early-access program at 29 French Innovative Leukemia Organization (FILO) centers, 63 (31%) were still on ibrutinib after 3 years and 57 provided a fresh blood sample. Thirty patients had a CLL clone ≥0.5 × 109/L, enabling next-generation sequencing (NGS); BTK and PLCG2 mutations were detected in 57% and 13% of the NGS samples, respectively. After median follow-up of 8.5 months from sample collection, the presence of a BTK mutation was significantly associated with subsequent CLL progression (P = .0005 vs no BTK mutation). Our findings support that mutational analysis should be considered in patients receiving ibrutinib who have residual clonal lymphocytosis, and that clinical trials are needed to evaluate whether patients with a BTK mutation may benefit from an early switch to another treatment.
Introduction
The Bruton tyrosine kinase (BTK) inhibitor ibrutinib has demonstrated efficacy in the treatment of chronic lymphocytic leukemia (CLL) in the relapsed/refractory1,2 and first-line3,4 settings. Long-term outcomes have mainly been evaluated in clinical trials.5-9 Data from real-life cohorts are only just starting to emerge.10-12
Mutational analyses performed following acquired ibrutinib resistance have suggested that CLL progression on ibrutinib is linked to mutations in the BTK and/or phospholipase Cγ2 (PLCG2) genes.13-19 However, mutational information for patients still on ibrutinib, without evidence of CLL progression, is limited.13,19 Uncertainty therefore remains about whether BTK and PLCG2 mutations directly cause, and are sufficient for, ibrutinib resistance.20
In France, ibrutinib became available as an early-access program (EAP) in 2014 and this has allowed its evaluation for prolonged use in a real-life cohort. Here, we report a study conducted by the French Innovative Leukemia Organization (FILO) Group that gives a “snapshot” of the prevalence of mutations in patients from the French EAP still on ibrutinib after at least 3 years of treatment.
Study design
Twenty-nine FILO centers provided data for all patients who initiated ibrutinib via the French EAP between February 2014 and April 2015 and were still on ibrutinib after 3 years. Fresh blood samples were taken and sent to the Avicenne laboratory (Assistance Publique–Hôpitaux de Paris [AP-HP], Bobigny, France) for central analyses. Flow cytometry techniques were used to determine presence of minimal residual disease, at a level of <1 CLL cell per 10 000 lymphocytes (<10−4),21 and to determine CLL cell counts. For samples exhibiting a CLL clone ≥0.5 × 109/L, mutational profiling by next-generation sequencing (NGS) was performed for BTK, PLCG2, TP53, NOTCH1, SF3B1, XPO1, RPS15, ATM, POT1, BIRC3, and FBXW7. All BTK C481S samples with variant allele frequency (VAF) <10% by NGS were confirmed by droplet digital polymerase chain reaction (ddPCR). Following sample collection, patients were followed for subsequent CLL progression (as assessed by the FILO local investigator) and treatment outcomes including event-free survival (event defined as a new treatment of CLL or death) and overall survival. Statistical analyses were by the Fisher exact test (for nominal variables) or the log-rank test (for survival outcomes).
The study was conducted in accordance with national ethical recommendations and the Declaration of Helsinki, and with written informed patient consent.
Additional study details are provided in the supplemental Study protocol and supplemental Methodological details (available on the Blood Web site).
Results and discussion
Of 204 patients who received ibrutinib via the French EAP at 29 FILO centers, 63 (31%) were still on ibrutinib after at least 3 years of treatment, and 57 provided fresh blood samples (supplemental Figure 1). Considering these 57 patients, the median time between ibrutinib initiation and sample collection was 3.5 years (range, 2.8-4.2 years) (Table 1). Most patients had adverse prognostic factors. All but 3 patients (each with 17p deletion) had received previous treatment (median 2 lines), usually including immunochemotherapy or alemtuzumab. Despite 3 years on ibrutinib, 13% of patients (7 of 55 with response data) had partial response with lymphocytosis22 and all 57 patients exhibited detectable minimal residual disease (>10−4).
Patient characteristics
| Characteristic | Result, N = 57* |
|---|---|
| Age at ibrutinib initiation, median (range), y | 67.7 (46.9-84.1) |
| Male/female, n/n, (ratio) | 39/18 (2.2) |
| Prognostic factors, n/N (%) | |
| 11q deletion | 18/40 (45) |
| 17p deletion | 20/47 (43) |
| Unmutated IGHV | 34/38 (89) |
| Previous lines, median (range) | 2 (0-5) |
| Previous lines, n (%) | |
| FCR or BR | 46 (81) |
| Alemtuzumab plus or minus dexamethasone | 9 (16) |
| Chlorambucil plus or minus anti-CD20 | 14 (25) |
| Other | 25 (44) |
| Best response on ibrutinib therapy, investigator reported, n/N (%) | |
| PR | 48/55 (87) |
| PRl | 7/55 (13) |
| Transient dose interruption >7 d, n/N (%) | 20/55 (37) |
| Dose reduction, n/N (%) | 23/55 (42) |
| Characteristic | Result, N = 57* |
|---|---|
| Age at ibrutinib initiation, median (range), y | 67.7 (46.9-84.1) |
| Male/female, n/n, (ratio) | 39/18 (2.2) |
| Prognostic factors, n/N (%) | |
| 11q deletion | 18/40 (45) |
| 17p deletion | 20/47 (43) |
| Unmutated IGHV | 34/38 (89) |
| Previous lines, median (range) | 2 (0-5) |
| Previous lines, n (%) | |
| FCR or BR | 46 (81) |
| Alemtuzumab plus or minus dexamethasone | 9 (16) |
| Chlorambucil plus or minus anti-CD20 | 14 (25) |
| Other | 25 (44) |
| Best response on ibrutinib therapy, investigator reported, n/N (%) | |
| PR | 48/55 (87) |
| PRl | 7/55 (13) |
| Transient dose interruption >7 d, n/N (%) | 20/55 (37) |
| Dose reduction, n/N (%) | 23/55 (42) |
BR, bendamustine plus rituximab; FCR, fludarabine plus cyclophosphamide plus rituximab; IGHV, immunoglobulin heavy chain variable gene; PR, partial response; PRl, partial response with lymphocytosis.
Except where otherwise stated.
Our study is original in providing a snapshot of the mutational profile of patients still on ibrutinib in the real-life setting at a definite long-term time point. Most previous mutational analyses were performed in patients with acquired ibrutinib resistance.13-19 To our knowledge, only 1 previous study prospectively examined BTK and PLCG2 mutations longitudinally; patients were recruited from 4 clinical trials and the data were published at a maximum 9-month time point.13 In our study, 30 blood samples exhibited a CLL clone ≥0.5 × 109/L, allowing mutational profiling by NGS (Figure 1A). The mutations detected were in line with previous reports in patients with acquired ibrutinib resistance, with no new mutations seen. One-half of the patients tested by NGS (15 of 30) had a TP53 mutation. At least 1 BTK mutation (total 20 mutations, all at C481, 14 at C481S) occurred in 17 of 30 patients (57%) and the VAF range was wide (0.2%-73%) (supplemental Table 1). ddPCR confirmation of C481S samples with negative or low VAF by NGS showed high concordance, with only 1 case detected by ddPCR (VAF, 0.37%) but not NGS (supplemental Table 2). Most patients (14 of 17) had a single BTK mutation, and there were no statistically significant associations between presence of a BTK mutation and the number of previous treatment lines (0 of 1 vs ≥2), need for transient interruptions or dose reductions (supplemental Table 3), or presence of any other mutations. At least 1 PLCG2 mutation (total 7 mutations) occurred in 4 of 30 patients (13%) and the VAF was low (1%-11%). Strikingly, 3 of the 4 patients had 2 PLCG2 mutations, and all 4 also presented with a BTK mutation and a TP53 mutation. The high prevalence of BTK mutations, with or without PLCG2 mutations, suggests that patients can harbor these mutations even when they are still benefiting clinically from ibrutinib. In support of this, the previous prospective longitudinal study reported that of 8 patients who experienced clinical relapse, all had a BTK mutation before relapse, and that a BTK mutation was also detected in 8 additional patients (the PLCG2 mutational status of patients was not stated).13 Furthermore, a retrospective analysis using stored samples from a clinical trial found that of 9 patients with a BTK and/or PLCG2 mutation detected at CLL progression, 6 had detectable mutations that predated the progression.19
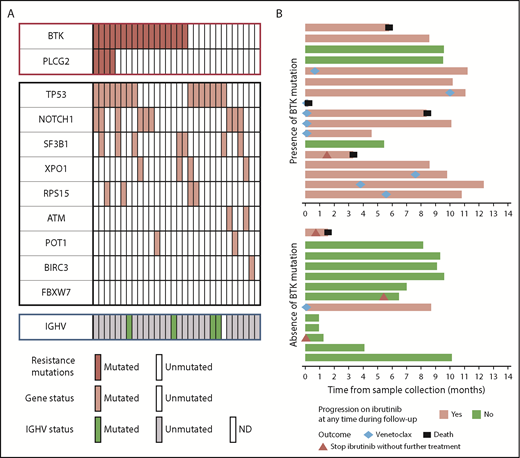
Findings in patients with CLL clone ≥0.5 × 109/L (N = 30). (A) Mutational profile, by NGS. Each column represents a patient. BTK mutations had no association with TP53 mutations or other mutations. PLCG2 mutations were all associated with BTK mutations and TP53 mutations. (B) Outcomes subsequent to sample collection in presence (n = 17) or absence (n = 13) of BTK mutations, with regard to CLL progression and treatment. Each bar represents a patient. IGHV, immunoglobulin heavy chain variable gene; ND, not determined.
Findings in patients with CLL clone ≥0.5 × 109/L (N = 30). (A) Mutational profile, by NGS. Each column represents a patient. BTK mutations had no association with TP53 mutations or other mutations. PLCG2 mutations were all associated with BTK mutations and TP53 mutations. (B) Outcomes subsequent to sample collection in presence (n = 17) or absence (n = 13) of BTK mutations, with regard to CLL progression and treatment. Each bar represents a patient. IGHV, immunoglobulin heavy chain variable gene; ND, not determined.
During the follow-up for subsequent CLL progression in our study, at a median 8.5 months from sample collection, only 38 patients (19% of the 204 initially treated) remained on ibrutinib. The drop from 28% at sample collection suggests that a noteworthy proportion of patients experience CLL progression between the third and fourth year on ibrutinib treatment. Considering the 27 patients with CLL clones <0.5 × 109/L, 4 subsequently progressed (supplemental Figure 2). Of 2 patients mutationally profiled at relapse, 1 had both BTK and PLCG2 mutations and the other had a BTK mutation only. By contrast, considering the 30 patients with a CLL clone ≥0.5 × 109/L, presence of a BTK mutation was significantly associated with subsequent CLL progression (P = .0005 vs no BTK mutation) (Figure 1B). Among the 17 patients with a BTK mutation, 14 subsequently progressed (1 had Richter syndrome): 3 progressors remained on ibrutinib, 9 received venetoclax (5 of 7 evaluable had an objective response), and 2 died without further treatment. Among the 13 patients with no BTK mutation, only 2 progressed: one died without further treatment and the other received venetoclax. The event-free survival was significantly shorter in patients with a BTK mutation (P = .0380 vs no BTK mutation), but there was no difference in terms of overall survival (supplemental Figure 3).
In conclusion, in this real-life CLL cohort of 57 patients still on ibrutinib after 3 years, over one-half of patients (57%) with a CLL clone ≥0.5 × 109/L had a BTK mutation, and presence of a BTK mutation conferred a greater likelihood of subsequent CLL progression. These findings support that mutational analysis should be considered in patients receiving ibrutinib who have residual clonal lymphocytosis, and that clinical trials are needed to evaluate whether patients with a BTK mutation may benefit from an early switch to another treatment. A new generation of noncovalent BTK inhibitor that does not interact with the BTK C481 site is of interest.23
Presented in abstract form at the 60th annual meeting of the American Society of Hematology, San Diego, CA, 1-4 December 2018.
For original data, please contact florence.cymbalista@aphp.fr.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
The authors thank Guillaume Cartron (Montpellier), Sophie De Guibert (Rennes), Charles Herbaux (Lille), Benedicte Hivert (Lens), Véronique Leblond (Paris Pitié Salpétrière), Katell le Du (Le Mans), Stéphane Leprètre (Rouen), Fathia Merabet (Versailles), David Sibon (Paris Necker), Malgorzata Truchan-Graczyk (Angers), and Maud Voldoire (La Roche sur Yon), who provided both clinicobiological information and samples from their patients. The authors thank Marie-Christine Bene (Nantes) for database creation. The authors thank Judy A. Fox and Pietro Taverna (Sunesis Pharmaceuticals, Inc) for reviewing and editing the manuscript.
This work was supported by Sunesis Pharmaceuticals, Inc and the Force Hemato (Fonds De Recherche Clinique en Hématologie) Foundation. Sunesis Pharmaceuticals, Inc kindly provided funding for the writing assistance.
Authorship
Contribution: A.Q., L.M.-F., F.C., and F.B.-M. conceived the study and wrote the manuscript; R.L., C.F., G.L., K.H., and F.B.-M. performed biological analyses; L.Y., M.-S.D., D.N., R.G., P.F., D.R.-W., L.W., A.-S.M., and A.D. provided blood samples and collected data from their patients; and V.L. performed statistical analyses.
Conflict-of-interest disclosure: A.Q., L.Y., R.G., A.-S.M., A.D., V.L., and F.C. declared travel grants and honoraria from Janssen, Gilead, Roche, and AbbVie. R.L. declared travel grants and honoraria from Janssen, Roche, and AbbVie. M.-S.D. declared travel grants and honoraria from Janssen and AbbVie. L.-M.F. declared travel grants and honoraria from Janssen, Gilead, and Roche. The remaining authors declare no competing financial interests.
A complete list of the members of the FILO CLL Group appears in "Appendix."
Correspondence: Anne Quinquenel, MCU-PH, Hématologie Clinique, CHU de Reims, Hôpital Robert Debré, Rue du général Koenig, 51092 Reims, France; e-mail: aquinquenel@chu-reims.fr.
Appendix: study group members
The members of the FILO CLL group are: Thérèse Aurran-Schleinitz (Marseille, France), F.B.-M., Marie-Christine Béné (Nantes, France), Fontanet Bijou (Bordeaux, France), Annie Brion (Besançon, France), R.G., Guillaume Cartron (Montpellier, France), Aline Clavert (Angers, France), F.C., A.D., M.-S.D., Sophie de Guibert (Rennes, France), Caroline Dartigeas (Tours, France), Bernard Drenou (Mulhouse, France), Jehan Dupuis (Creteil, France), Emmanuelle Ferrant, P.F., C.F., L.M.-F., David Ghez (Villejuif), R.G., Charles Herbaux (Lille, France), Kamel Laribi (Le Mans, France), G.L., Katell Le Du (Le Mans, France), Magali Le Garff Tavernier (Paris, France), Véronique Leblond (Paris, France), Stephane Lepretre (Rouen, France), R.L., V.L., Béatrice Mahé (Nantes, France), Karim Maloum (Paris, France), Marc Maynadié (Dijon, France), Fatiha Merabet (Versailles, France), A.-S.M., Pierre Morel (Amiens, France), Florence Nguyen Khac (Paris, France), D.N., Brigitte Pégourie (Grenoble, France), Bertrand Pollet (Boulogne sur Mer, France), Stéphanie Poulain (Valenciennes, France), A.Q., Sophie Raynaud (Nice, France), Daniel Ré (Antibes, France), Philippe Rodon (Périgueux, France), D.R.-W., Valérie Rouille (Montpellier, France), Laurence Sanhes (Perpignan, France), Laurence Simon (Corbeil-Essonnes, France), Cécile Tomowiak (Poitiers, France), David Sibon (Paris, France), Olivier Tournilhac (Clermont Ferrand, France), Xavier Troussard (Caen, France), Malgorzata Truchan-Graczyk (Angers, France), Eric Van Den Neste (Bruxelles, France), Sandrine Vaudaux (Rouen, France), Marguerite Vignon (Paris, France), Jean-Pierre Vilque (Caen, France), Maud Voldoire (La Roche sur Yon, France), L.W., L.Y., and Jean-Marc Zini (Paris, France).

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal