

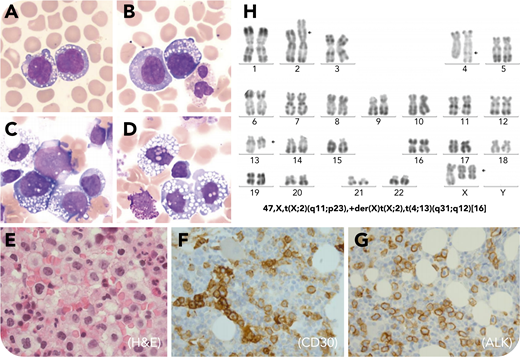
A 25-year-old woman presented with fever, retroperitoneal and inguinal adenopathy, and a skin rash with erythematous lesions on the trunk and legs. The absolute lymphocyte count was increased at 7 × 109/L. Examination of the blood (panels A-B: May-Grünwald Giemsa stain, ×100 objective, total magnification ×1000) and bone marrow aspirate smears (panels C-D: May-Grünwald Giemsa stain, ×100 objective, total magnification ×1000) revealed large cells with an abundant gray-blue vacuolated cytoplasm, reticular chromatin, and convoluted, folded nuclei. Flow cytometry of the blood detected large cells CD3+CD4+CD25+ and was negative for CD7, CD8, CD16, and CD56 markers. Immunohistochemistry analysis of the bone marrow, lymph nodes, and skin biopsies established the diagnosis of anaplastic large cell lymphoma (ALCL), CD4+CD3+CD5+CD30+, and EMA+, demonstrating an unusual cell membrane-restrictive ALK immunostaining (panel E: hematoxylin and eosin stain, ×100 objective, total magnification ×1000; panels F-G: CD30 and ALK stain, ×40 objective, total magnification ×400). Epstein-Barr virus, CD15, and CD20 were negative. An identical clonal rearrangement of the TCRG gene was detected in the bone marrow, skin, and lymph node biopsies. Conventional cytogenetic studies of the bone marrow aspirate demonstrated a complex karyotype including the rare variant translocation t(X;2)(q11;p23) (panel H). Prognosis of patients with leukemic ALCL is usually very poor. Indeed, the patient died of bacterial meningitis rapidly after the first cyclophosphamide, doxorubicin, vincristine, and prednisone–based chemotherapy course.
The membrane retention of ALK observed in this case is the result of the translocation t(X;2), which fuses ALK to MSN, a gene encoding for a membrane-restricted protein. Thus, the translocation t(X;2) should be sought when this pattern of ALK staining is observed. This case also illustrates the great variability in morphologic presentation of ALCL, which can at times resemble monocytoid/monoblastic cells.
A 25-year-old woman presented with fever, retroperitoneal and inguinal adenopathy, and a skin rash with erythematous lesions on the trunk and legs. The absolute lymphocyte count was increased at 7 × 109/L. Examination of the blood (panels A-B: May-Grünwald Giemsa stain, ×100 objective, total magnification ×1000) and bone marrow aspirate smears (panels C-D: May-Grünwald Giemsa stain, ×100 objective, total magnification ×1000) revealed large cells with an abundant gray-blue vacuolated cytoplasm, reticular chromatin, and convoluted, folded nuclei. Flow cytometry of the blood detected large cells CD3+CD4+CD25+ and was negative for CD7, CD8, CD16, and CD56 markers. Immunohistochemistry analysis of the bone marrow, lymph nodes, and skin biopsies established the diagnosis of anaplastic large cell lymphoma (ALCL), CD4+CD3+CD5+CD30+, and EMA+, demonstrating an unusual cell membrane-restrictive ALK immunostaining (panel E: hematoxylin and eosin stain, ×100 objective, total magnification ×1000; panels F-G: CD30 and ALK stain, ×40 objective, total magnification ×400). Epstein-Barr virus, CD15, and CD20 were negative. An identical clonal rearrangement of the TCRG gene was detected in the bone marrow, skin, and lymph node biopsies. Conventional cytogenetic studies of the bone marrow aspirate demonstrated a complex karyotype including the rare variant translocation t(X;2)(q11;p23) (panel H). Prognosis of patients with leukemic ALCL is usually very poor. Indeed, the patient died of bacterial meningitis rapidly after the first cyclophosphamide, doxorubicin, vincristine, and prednisone–based chemotherapy course.
The membrane retention of ALK observed in this case is the result of the translocation t(X;2), which fuses ALK to MSN, a gene encoding for a membrane-restricted protein. Thus, the translocation t(X;2) should be sought when this pattern of ALK staining is observed. This case also illustrates the great variability in morphologic presentation of ALCL, which can at times resemble monocytoid/monoblastic cells.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal