

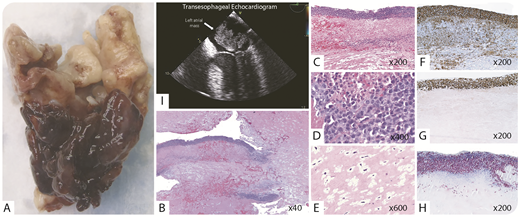
An immunocompetent 50-year-old man presented with chest pain. An echocardiogram showed a left atrial mass, which was resected (panel I). Macroscopically, there was a 6-cm gelatinous mass with a friable tissue rim (panel A). Microscopically, it was predominately composed of spindle cells in a myxoid stroma (panels B and E; hematoxylin and eosin stain); however, the rim consisted of large lymphoma cells with numerous mitoses and necrosis (panels B-D; hematoxylin and eosin stain). Immunohistochemically, the lymphoma cells were positive for CD20 (panel F; CD20 stain) and MUM-1, and negative for CD10. The Ki-67 proliferation rate was 90% (panel G; Ki-67 stain) and in situ hybridization of Epstein-Barr virus (EBV)-encoded RNA (EBER) was positive (panel H; EBER stain). The diagnosis was fibrin-associated diffuse large B-cell lymphoma (FA-DLBCL). Staging workup was negative in all other sites. The patient declined chemotherapy, and, after 65 months, he remains without evidence of recurrence.
FA-DLBCL is a rare subtype of EBV+ DLBCL typically detected incidentally in immunocompetent patients during the examination of fibrin-rich pathology specimens, including cardiovascular prostheses, thrombi, and myxomas. Unlike pyothorax-associated lymphoma, which is the prototype of DLBCL associated with chronic inflammation, FA-DLBCL tends to be confined to the primary disease site, and the clinical outcome is highly favorable, even with surgical excision alone.
An immunocompetent 50-year-old man presented with chest pain. An echocardiogram showed a left atrial mass, which was resected (panel I). Macroscopically, there was a 6-cm gelatinous mass with a friable tissue rim (panel A). Microscopically, it was predominately composed of spindle cells in a myxoid stroma (panels B and E; hematoxylin and eosin stain); however, the rim consisted of large lymphoma cells with numerous mitoses and necrosis (panels B-D; hematoxylin and eosin stain). Immunohistochemically, the lymphoma cells were positive for CD20 (panel F; CD20 stain) and MUM-1, and negative for CD10. The Ki-67 proliferation rate was 90% (panel G; Ki-67 stain) and in situ hybridization of Epstein-Barr virus (EBV)-encoded RNA (EBER) was positive (panel H; EBER stain). The diagnosis was fibrin-associated diffuse large B-cell lymphoma (FA-DLBCL). Staging workup was negative in all other sites. The patient declined chemotherapy, and, after 65 months, he remains without evidence of recurrence.
FA-DLBCL is a rare subtype of EBV+ DLBCL typically detected incidentally in immunocompetent patients during the examination of fibrin-rich pathology specimens, including cardiovascular prostheses, thrombi, and myxomas. Unlike pyothorax-associated lymphoma, which is the prototype of DLBCL associated with chronic inflammation, FA-DLBCL tends to be confined to the primary disease site, and the clinical outcome is highly favorable, even with surgical excision alone.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal