

Abstract
Background:
Leukemia stem cells (LSCs) play a critical role in AML propagation and relapse. Other investigators have also highlighted unique gene expression profiles for the leukemia stem cell population. Here we compared the results of in vitro drug sensitivity testing against a custom panel of drugs and drug combinations for blast populations vs. leukemia stem cell populations derived from the same patients, as well as mutation analysis for a panel of 194 recurrently mutated genes in AML.
Patients and Methods:
Patient AML samples were obtained with IRB approval. LSCs were isolated by fluorescence-activated cell sorting (FACS) and the blast population enriched to >90% using immunomagnetic beads from blood samples from 5 patients with AML. A sixth AML patient sample was used for NOD/SCID IL2R γc−/− engraftment, in order to compare characteristics of pre- and post-engraftment subclones. Our CLIA approved custom assay includes 153 drugs and targeted agents, both FDA approved and investigational, with additional drug combinations. High throughput screens (HTS) were conducted with enriched cells adherent to matrix protein in 384 well plates with 8 concentrations of each drug spanning 4 logs. Viability was assessed with CellTiter-Glo (Promega). HTS were performed on LSCs, blasts and pre- as well as post-engraftment AML subclones from the xenograft. Dose-response curves were generated to calibrate drug resistance patterns. Mutation analysis by NGS for a panel of 194 recurrently mutated genes in AML (MyAML®) including 37 translocations was also conducted for the LSC and blast populations.
Results:
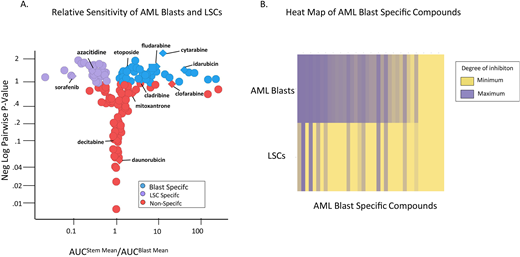
AML blasts and LSCs exhibited divergent drug susceptibility patterns (see volcano plot in Figure). Of 11 drugs commonly used in AML, 8 were typical chemotherapy drugs. Five of these compounds were effective against blasts, but none were effective against LSCs (p-value: 0.0256), suggesting a possible mechanism for post-treatment relapse or primary refractoriness. LSCs were also resistant to mitomycin-C, an agent that induces DNA interstrand crosslinks and DNA breaks, in contrast to blasts that were variably sensitive. Of note, we identified 12 drugs from 8 classes defined by mechanism of action that may target LSCs, in some cases preferentially, when compared with blasts. Drugs effective in preferentially targeting LSCs included tyrosine kinase inhibitors, histone deacetylase inhibitors, 1 cyclin-dependent kinase inhibitor, 1 proteasome inhibitor and 1 microtubule assembly inhibitor. Several of the drugs that efficiently killed LSCs have been studied clinically in AML, while others have theoretical or established efficacy against LSCs by drug class. Only one commonly used drug in AML, sorafenib, a multikinase inhibitor used in FLT3+ disease that may improve survival in younger patients, was effective against LSCs. Blast specific drugs include romidepsin, dinaciclib, alvocidib, ganetespib, selinexor, dorsomorphin, vinblastine, cladribine, dabrafenib, selumetinib, etoposide, torkinib and those in Figure. Blast and LSC drug susceptibility patterns were distinct for each patient.
Further, the engrafted xenograft subclone grew very rapidly, was resistant to standard chemotherapy, and possessed three new deleterious mutations in KMT2C (2), SF3B1 and 1 possibly damaging mutation in NUP214, suggesting possible genetic contributions to chemotherapy resistance. We also compared mutation profiles for LSCs vs. blasts in 5 patients, and identified LSC specific mutations in WNK3, WNK4 and BUB1, each in 2 of the 5, and there were also other mutations that were LSC or blast specific. Of note, Bub1 is a mitotic checkpoint serine/threonine kinase that controls mitosis in cancer stem cells (Venere et al Cancer Discov. 2013). WNK3 and WNK4 also both encode serine/threonine protein kinases.
Conclusions:
The distinct drug susceptibility patterns of patient-specific LSC and blast populations highlight the potential of an individualized approach to treat AML. LSCs are resistant to S-phase agents used in standard-of-care chemotherapy. Genetically distinct minority resistant LSC subclones present at diagnosis may grow rapidly under some conditions, and contribute to drug resistance and relapse. Incorporating the results of functional drug screening focused on LSC subclones may allow more individualized treatment of AML patients and identify patient-specific therapies that lead to improved outcomes.
Carson:Invivoscribe Inc.: Employment. Patay:Invivoscribe Inc.: Consultancy, Equity Ownership, Patents & Royalties. Becker:Novartis: Research Funding; Trovagene: Research Funding; CVS Caremark: Consultancy; JW Pharmaceuticals: Research Funding; Rocket Pharmaceuticals: Research Funding; Pfizer: Consultancy; Amgen: Research Funding; BMS: Research Funding; Abbvie: Research Funding; GlycoMimetics: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal