

A 62-year-old woman was investigated for myeloproliferative neoplasm with splenomegaly. Complete blood count showed the following: hemoglobin, 123 g/L; leukocytes, 30.7 × 109/L; platelets, 273 × 109/L; myelocytes, 1.14 × 109/L; neutrophils, 23.72 × 109/L; eosinophils, 0.43 × 109/L; and basophils, 1.02 × 109/L. She had no skin lesions/lymphadenopathy, but lactate dehydrogenase was elevated (416 U/L). Peripheral blood (PB) showed a leukoerythroblastosis with teardrops and rare blasts. Aspirate was unsuccessful. Biopsy was hypercellular with megakaryocytic hyperplasia and atypia (panel A; original magnification ×40, hematoxylin and eosin stain) and focally increased eosinophils and MF-3 fibrosis (panel B; original magnification ×40, reticulin stain). CD34 showed <1% blasts. CD117 highlighted multifocal infiltrates of spindle-shaped/atypical mast cells (≥15) in aggregates (panel C; original magnification ×40) with positive tryptase/CD25 (panel D; original magnification ×40). JAK2 was positive and c-Kit on PB and BCR-ABL was negative. These findings fulfilled the major and 2 minor criteria for systemic mastocytosis (SM) and the 3 major and 4 minor criteria for overt primary myelofibrosis (PMF). The diagnosis was consistent with SM with an associated hematological neoplasm (SM-AHN) per 2016 World Health Organization criteria.
Compared with other SM-AHN, SM with associated PMF is relatively rare, likely because it can be easily missed as a result of dry tap and fibrosis. The case highlights the importance of careful inspection of biopsy and applying CD117 staining initially to unfold the disguised SM-AHN.
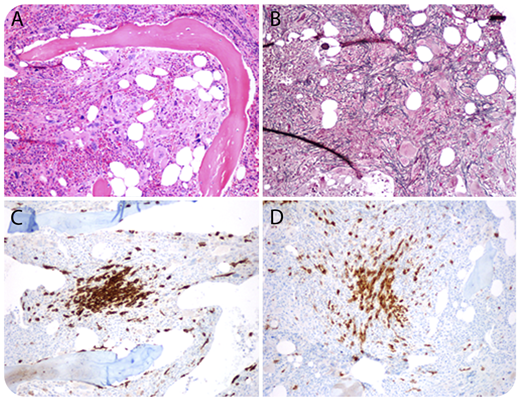
A 62-year-old woman was investigated for myeloproliferative neoplasm with splenomegaly. Complete blood count showed the following: hemoglobin, 123 g/L; leukocytes, 30.7 × 109/L; platelets, 273 × 109/L; myelocytes, 1.14 × 109/L; neutrophils, 23.72 × 109/L; eosinophils, 0.43 × 109/L; and basophils, 1.02 × 109/L. She had no skin lesions/lymphadenopathy, but lactate dehydrogenase was elevated (416 U/L). Peripheral blood (PB) showed a leukoerythroblastosis with teardrops and rare blasts. Aspirate was unsuccessful. Biopsy was hypercellular with megakaryocytic hyperplasia and atypia (panel A; original magnification ×40, hematoxylin and eosin stain) and focally increased eosinophils and MF-3 fibrosis (panel B; original magnification ×40, reticulin stain). CD34 showed <1% blasts. CD117 highlighted multifocal infiltrates of spindle-shaped/atypical mast cells (≥15) in aggregates (panel C; original magnification ×40) with positive tryptase/CD25 (panel D; original magnification ×40). JAK2 was positive and c-Kit on PB and BCR-ABL was negative. These findings fulfilled the major and 2 minor criteria for systemic mastocytosis (SM) and the 3 major and 4 minor criteria for overt primary myelofibrosis (PMF). The diagnosis was consistent with SM with an associated hematological neoplasm (SM-AHN) per 2016 World Health Organization criteria.
Compared with other SM-AHN, SM with associated PMF is relatively rare, likely because it can be easily missed as a result of dry tap and fibrosis. The case highlights the importance of careful inspection of biopsy and applying CD117 staining initially to unfold the disguised SM-AHN.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal