

In this issue of Blood, report the final results of the phase 3 registration trial DUO,1 which compared the novel PI3Kδ,γ inhibitor duvelisib with ofatumumab in patients with relapsed refractory chronic lymphocytic leukemia (CLL) and demonstrated a significant improvement in progression-free survival (PFS) with duvelisib. On 24 September 2018, these results led to US Food and Drug Administration (FDA) approval of duvelisib for the therapy of CLL patients after ≥2 prior regimens.
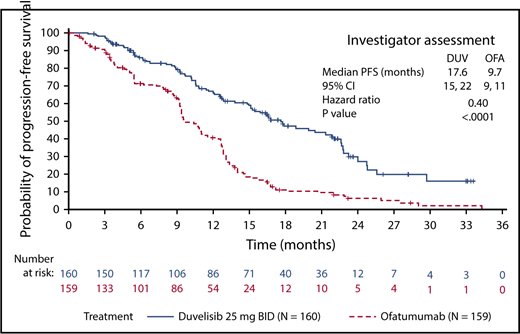
Progression-free survival in DUO per investigator assessment, comparing duvelisib with ofatumumab. BID, twice a day; DUV, duvelisib; OFA, ofatumumab. See the complete Figure 1 in the article by Flinn et al that begins on page 2446.
Progression-free survival in DUO per investigator assessment, comparing duvelisib with ofatumumab. BID, twice a day; DUV, duvelisib; OFA, ofatumumab. See the complete Figure 1 in the article by Flinn et al that begins on page 2446.
Over the last several years, the excitement about targeted agents in CLL has continued to build, with FDA approvals for ibrutinib in frontline therapy and venetoclax with rituximab for relapsed disease. Very early data on combinations, focused particularly on ibrutinib with venetoclax, are also starting to emerge. In the midst of this whirlwind, the role of PI3Kδ inhibitors has been murky, particularly since 2016 when Gilead Sciences terminated multiple early-line combination trials of idelalisib due to an excess of infectious deaths. Since then, copanlisib, a pan-PI3K inhibitor, has received accelerated approval for the therapy of follicular lymphoma after ≥2 prior regimens,2 but to date has had limited study in CLL.
Into this mix comes duvelisib, a potent and specific inhibitor of PI3Kδ, as well as PI3Kγ. The significance of γ isoform inhibition is not clear, but interest has focused on its potential role in modulating macrophage and T-cell function in the microenvironment,3 which may reduce survival support to CLL cells or help generate an antitumor immune response. This hypothesis is supported by decreases in CLL-derived and microenvironment-derived cytokines during duvelisib therapy4,5 and preliminary correlations of these alterations with duration of response.4
What about the clinical data? In the phase 1 study in heavily pretreated CLL patients, duvelisib showed a 56% overall response rate by International Workshop on Chronic Lymphocytic Leukemia criteria and a median PFS of 15.7 months across all dose levels.5 In the phase 3 DUO study reported here by Flinn et al, 319 patients with a median of 2 prior regimens were randomized to duvelisib or ofatumumab; about 70% of patients had unmutated IGHV and 30% had 17p deletion. With a median follow-up of 22.4 months, the median PFS by independent review committee was 13.3 months with duvelisib vs 9.9 months with ofatumumab, whereas the median investigator-assessed PFS was 17.6 months with duvelisib vs 9.7 months with ofatumumab. The source of this discrepancy is not detailed in the article, but the investigator-assessed PFS with single-agent duvelisib (see figure) actually looks quite similar to the PFS of idelalisib with anti-CD20 antibody in its registration trials.6,7
As exemplified by the idelalisib experience, the key issue with PI3Kδ inhibitors is managing toxicity over time. Adverse events were the primary reason for discontinuation of duvelisib in DUO, affecting 35% of patients, compared with 22% who discontinued for progressive disease. The side effect profile of duvelisib appears similar to idelalisib in a similar clinical setting,8 although transaminitis and pneumonitis were less common in DUO, at 3% each. As with idelalisib, the greatest concerns are immune-mediated side effects, particularly diarrhea and colitis, as well as potentially fatal infections. Protocol-specified management outlined in Flinn et al, including holding duvelisib early at the first sign of significant diarrhea or pneumonia, and the use of steroids or dose reductions as needed, should also be implemented in clinical practice. Prophylaxis against opportunistic infections is essential, as well as monitoring for and avoiding neutropenia through the use of myeloid growth factors. With appropriate vigilance and patient selection discussed below, PI3Kδ inhibitors can be safe and tolerable.
What then is the place of a PI3K inhibitor in current CLL therapy? PI3K inhibitors can be safely used in patients with significant cardiac comorbidities or the need for anticoagulation that limit the use of Bruton tyrosine kinase (BTK) inhibitors, as well as in patients with significant renal dysfunction that limits the use of venetoclax. Furthermore, the autoimmune toxicities of PI3Kδ inhibitors are age dependent and are worse in younger patients.9,10 They are also worse in previously untreated patients9,10 ; hence, the FDA approval of duvelisib in CLL patients with ≥2 prior therapies. Therefore, the ideal duvelisib candidate is an older patient with multiple prior therapies who has had BTK or BCL-2 inhibitors or has comorbidities precluding their use. Duvelisib has the advantage of being a single-agent oral drug not requiring the intense initial monitoring of venetoclax and, therefore, will be quite acceptable to this patient population.
The approval of duvelisib opens important avenues for further investigation. For example, although PI3K inhibitors are a potentially good option in patients whose disease has progressed on BTK or BCL-2 inhibitors, data are lacking on response rates and durability in that context. Combination studies are also ongoing; at Dana-Farber Cancer Institute, we are studying duvelisib with venetoclax (NCT03534323), and interest is high in (carefully) exploring combinations with other immunomodulatory agents. Multiple additional PI3Kδ inhibitors are also advancing in the clinic; these include umbralisib, which also inhibits casein kinase 1ε, as well as ME-401 and INCB50465, both of which are being explored on intermittent schedules in hopes of reducing toxicity. Ongoing translational studies to elucidate the immunomodulatory effects of PI3Kδ inhibitors will also start to inform their optimal clinical use. The approval of duvelisib will invigorate research to understand and optimally use this highly active, but complicated, drug class, both in CLL as more patients come off BTK and BCL-2 inhibitors, and in other diseases.
Conflict-of-interest disclosure: J.R.B. has consulted for Verastem Oncology, Gilead Sciences, TG Therapeutics, Janssen, Pharmacyclics, AbbVie, Genentech, Acerta Pharma, AstraZeneca, BeiGene, Loxo Oncology, Sunesis Pharmaceuticals, Sun Pharma, Pfizer, Celgene, Kite Pharma, Redx Pharma, and Astellas Pharma; has received an honorarium from Teva Pharmaceutical Industries and research funding from Verastem Oncology, Gilead Sciences, Sun Pharma, and Loxo Oncology; and has served on Data Safety Monitoring Boards for MorphoSys and Invectys.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal