

Abstract
Abstract 3040
We have previously shown that both lymphocyte and monocyte recovery are strongly associated with improved survival post-myeloablative allogeneic hematopoietic stem cell transplant for acute leukemia (Thoma et al, Biology of Blood and Marrow Transplantation, in press). We hypothesized that rapid lymphocyte and monocyte recovery would have a similarly positive impact on overall survival in reduced intensity conditioning (RIC) HSCT with fludarabine/melphalan. To test our hypothesis, we analyzed 118 consecutive patients who underwent allogeneic HSCT with fludarabine/melphalan conditioning for AML (n=49) and MDS/MPN (n=38), ALL (n=7) and other lymphoid malignancies (n=24) at our institution from 2001–2010. The absolute lymphocyte counts and monocyte counts (ALC and AMC, respectively) derived from routine complete blood counts were determined longitudinally at days +15, +30, +60, +100 and correlated with clinical outcomes. At the day +30 time point, both ALC and AMC > 0.3 × 10(9) cells/L were strongly associated with improved survival (OS 29.6 months vs. 5.4 months, p=0.006 and 25.3 months vs. 5.1 months, p=0.01 respectively), a pattern that continued through the day +100 evaluation. Multivariate analysis including age, CD34+ cell dose, unrelated vs. related HSCT, presence of aGVHD, remission status, and longitudinal hematologic parameters revealed that day +100 ALC (RR 0.21, 95% CI 0.07–0.66, p= 0.0096) and day +100 AMC (RR 0.41, 95% CI 0.2–0.9, p=0.047) were the only independent predictors of survival in the model. Pairwise correlations showed moderate negative associations between aGVHD and day +60 and day +100 ALC and AMC. To further explore whether any inherent patterns in the timing of lymphocyte and monocyte recovery had prognostic value post-HSCT, we performed unsupervised hierarchical clustering on the longitudinal hematopoietic parameters studied in this cohort and identified four clusters of patients, clusters A-D. Patient clusters A and C both demonstrated improved ALC and AMC recovery at the day +60 and day +100 time points and had significantly improved OS compared with clusters B and D (not reached for A and C vs. 54.9 and 22.3 months, respectively, p<0.001). No patient in cluster D had a day +100 AMC > 0.3 × 10(9) cells/L, and these patients experienced more acute GVHD (p=0.006) and relapse (8 of 14 patients, p=0.002) compared with clusters A, B, and C (p=0.002). 29 patients who were unable to be clustered with this algorithm, predominantly due to early toxic deaths, had a median survival of 6 months. Consistent with previous observations in our myeloablative cohort, both lymphocyte and monocyte recovery are predictive of overall survival post-RIC HSCT. However, compared to the myeloablative cohort, monocyte recovery in this series appears slightly less strongly associated with survival. Our results also extend the observation of improved survival of ALC and AMC recovery post-HSCT to diseases beyond acute leukemia.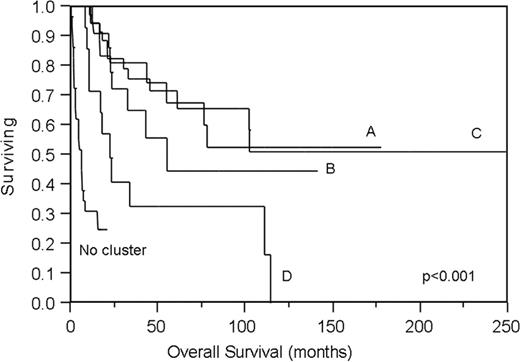

Disclosures:
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal