

Abstract
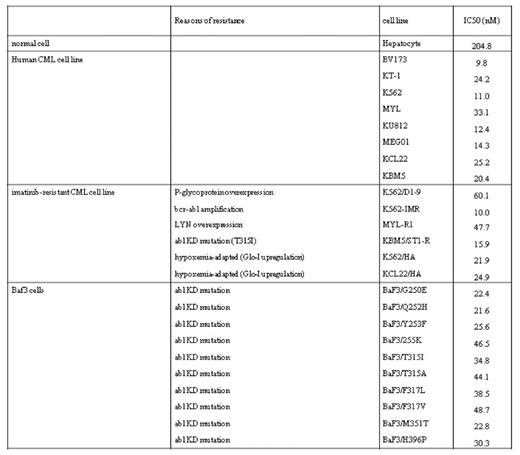
Imatinib and the second-generation ABL tyrosine kinase inhibitors (TKIs) such as dasatinib and nilotinib have dramatically changed the management of CML. However, these agents are effective neither for CML cells harboring T315I mutation nor for CML stem cells. Genetic analysis of blasts from CML patients in blast crisis has identified numerous members of the Wnt/b-catenin pathway as being activated (Radich et al, PNAS 2006) and loss of b-catenin has been reported to impair the renewal of CML stem cells (Chao et al, Cancer Cell 2007). Thus, b-catenin signaling inhibition may be useful for CML treatment. We herein describe the effects of a novel b-catenin inhibitor, AV65 on various imatinib-sensitive and –resistant CML cell lines (Table 1). Eight imatinib-sensitive human CML cell lines and one normal cell line derived from hepatocyte were exposed to AV65 for 72 hours and its anti-proliferative effects were examined by MTT assay. AV65 induced apoptosis in these CML cell lines time- and does-dependent manners and inhibited the growth of all eight CML cell lines with IC50 at ranging from 9.8 to 33.1nM. While that for hepatocyte was 204.8nM. Interestingly, AV65 induced polyploidies in K562 but not in BV173. In addition, AV65 augmented the anti-proliferative effects of imatinib additively against K562 and BV173. These findings suggested that AV65 alone or the combination with imatinib was effective for imatinib-sensitive CML cells. To investigated the effects of AV65 against imatinib-resistant CML cells, four imatinib-resistant CML cell lines such as K562/IMR (bcr-abl amplification), MYL-R1 (LYN overexpression), KBM5/ STIR (harboring T315I) and K562/D1-9 (P-glycoprotein overexpression), and BaF3 cells expressing the wild type BCR-ABL or its ten different mutant BCR-ABL forms including T315I, were used. There was little difference on the induction of apoptosis and anti-proliferative effects of AV65 except K562/D1-9 between each parental cell line and its resistant clone and AV65 inhibited the growth of all examined BaF3 cells harboring various mutations including T315I with IC50 at ranging from 21.6 to 46.5nM. IC50 values of AV65 for K562 and K562/D1-9 were 11.0 and 60.1nM, respectively. These findings suggested that the effects of AV65 were independent either to BCR-ABL expression level, ABL mutations or LYN overexpression, but might be affected by P-glycoprotein. Next, the effects of AV65 against the hypoxia-adapted CML cell lines such as K562/ HA and KCL22/HA were also investigated. These cell lines were resistant to imatinib, dasatinib, INNO-406 (another second-generation ABL TKI; Kimura et al, Blood 2005) and alkylating agents via the up-regulation of glyoxalase-I, a detoxification enzyme for the cytotoxic byproducts of glycolysis. Intriguingly, AV65 inhibited the growth of hypoxiaadapted CML cell lines at almost same concentration compared with their parental cell lines. Although CML stem cell niche has not been definitely identified, it might located in hypoxia because the inoculated human leukemia cells to immunodeficient mice preferably localized on the surface of osteoblasts in the epiphysis (Ninomiya et al, Leukemia 2007) where could be hypoxic. Taken together, AV65 may be effective for CML stem cells in hypoxia. In conclusion, AV65 inhibited the growth of CML cell lines which acquire imatinib-resistance because of Abl kinase domain mutations including T315I and hypoxiaadaptation. Therefore, AV65 may become a promising agent for CML treatment including both imatinib and the second-generation Abl TKIs-resistant patients.
Figure
Disclosures: Strovel:Avalon pharmaceuticals: Employment. Cholody:Avalon pharmaceuticals: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal